
Estimated reading time: 10 minutes
LDL-P: A Better Marker of Cardiovascular Risk than LDL-C
Cholesterol numbers can appear normal, yet cardiovascular risk may still be elevated.
Standard blood tests typically report LDL-cholesterol (LDL-C), also known as the “bad cholesterol.” When this number falls within the target range, patients and clinicians often assume that the risk of heart disease is low. But this assumption can be misleading.
The key metric that’s often overlooked is LDL-P — low-density lipoprotein particle number. LDL-P reflects the actual number of LDL particles circulating in the blood. And it turns out that this number may be a more reliable indicator of cardiovascular risk than LDL-C alone.
A person can have low LDL-C but high LDL-P and remain at significant risk for atherosclerosis and cardiovascular events.
This article explores what LDL-P is, how it differs from LDL-C, why the number of particles matters, and how this metric can offer a more accurate understanding of heart disease risk.

What is LDL-P?
LDL-P stands for low-density lipoprotein particle number. It refers to the actual count of LDL particles in the bloodstream, not the amount of cholesterol they carry, but how many discrete particles are present.
Each LDL particle is capable of crossing the arterial wall and contributing to plaque formation. Therefore, a higher number of particles increases the likelihood of atherosclerosis, regardless of the total cholesterol content.
While standard tests measure LDL-C (the concentration of cholesterol within LDL particles), LDL-P quantifies the number of atherogenic units in circulation. This distinction is clinically important, as individuals with the same LDL-C may have very different LDL-P values, depending on particle size and number.
LDL-P vs. LDL-C: What’s the Difference?
Although often used interchangeably, LDL-P and LDL-C measure fundamentally different things.
-
LDL-C quantifies the amount of cholesterol carried by LDL particles.
-
LDL-P measures the number of LDL particles in the bloodstream.
Think of LDL-C as the total weight of cargo, and LDL-P as the number of trucks on the road. A person could have fewer large particles or many small ones. Both patterns can produce the same LDL-C value but represent very different risk profiles.
The term discordance refers to situations where LDL-C and LDL-P levels diverge from each other. Studies have shown that when such discordance exists, LDL-P is more closely associated with cardiovascular outcomes.
Up to 30–40% of individuals with low or normal LDL-C have elevated LDL-P — a finding that reveals hidden risk not captured by standard panels.

What About ApoB?
Apolipoprotein B (apoB) is a protein found on the surface of all atherogenic lipoproteins, including LDL, VLDL, IDL, and Lp(a). Since each particle carries exactly one molecule of apoB, the apoB concentration in blood reflects the total number of atherogenic particles, including LDL.
ApoB and LDL-P are therefore closely related, and both offer better predictive value for cardiovascular risk than LDL-C.
-
LDL-P measures the number of LDL particles specifically.
-
ApoB captures the total number of all atherogenic particles (LDL + others).
In most individuals, apoB and LDL-P correlate closely. However, apoB has the advantage of being more widely available, less costly, and easier to standardize. It is now increasingly used in risk assessment and as a treatment target.
Both apoB and LDL-P reflect particle number — not cholesterol mass — and thus more accurately assess atherogenic potential than LDL-C.
If you enjoy DocsOpinion’s longform articles, you may also like my Substack newsletter — shorter reflections, serialized essays, and behind-the-scenes notes on medicine, history, and science.
No spam. Unsubscribe anytime.
Why LDL-P Matters More for Heart Risk
Atherosclerosis is initiated and driven by the accumulation of lipoprotein particles in the arterial wall. Among these, LDL particles play a central role.
Each LDL particle can cross the endothelium, deposit cholesterol into the intima, and promote plaque development. The more particles present, the more frequently this process occurs, regardless of cholesterol content per particle.
When LDL-C and LDL-P are discordant, clinical outcomes tend to follow LDL-P. This makes LDL-P a stronger predictor of cardiovascular events, particularly in individuals with metabolic dysfunction characteristics.
How Is LDL-P Measured?
LDL-P is measured using nuclear magnetic resonance (NMR) spectroscopy, a specialized test that directly counts LDL particles, reporting results in nanomoles per liter (nmol/L).
This method provides a more precise estimate of the atherogenic burden than standard cholesterol testing. Despite its clinical value, LDL-P is not routinely assessed in most lipid panels and is underutilized in general practice.
What Affects LDL-P?
LDL-P levels are influenced by several metabolic factors, especially those associated with insulin resistance.
Elevated triglycerides are a key driver. High triglyceride levels lead to increased production of very-low-density lipoproteins (VLDL), which are metabolized into smaller, denser LDL particles. This results in a greater number of particles, even when total cholesterol remains unchanged.
Conditions commonly associated with elevated LDL-P include:
- High triglycerides
- Low HDL-C
- Insulin resistance or type 2 diabetes
- Central obesity
- Non-alcoholic fatty liver disease (NAFLD)
Additional contributors include:
- High intake of refined carbohydrates
- Sedentary lifestyle
- Weight gain (especially visceral fat)
- Hypothyroidism
- Chronic kidney disease
- Genetic predispositions (e.g., familial combined hyperlipidemia)
- Lipid profiles showing high triglycerides and low HDL-C should prompt consideration of elevated LDL-P, even if LDL-C appears normal.
How to Lower LDL-P
Reducing LDL particle number (LDL-P) involves more than just targeting cholesterol levels — it requires addressing both lipid metabolism and underlying metabolic dysfunction. This means combining lifestyle strategies with pharmacological options when necessary.
Lifestyle and Dietary Strategies
These interventions aim to reduce hepatic lipoprotein production, improve insulin sensitivity, and lower triglyceride-rich lipoproteins — all of which influence LDL-P:
- Adopt a Low-Carbohydrate or Mediterranean-Style Diet
Both dietary patterns have been shown to lower LDL-P, particularly in those with insulin resistance. Low-carb diets reduce hepatic VLDL production by lowering insulin and de novo lipogenesis. Mediterranean diets, rich in monounsaturated fats and fiber, also improve lipid profiles and metabolic parameters. - Lose Visceral Fat
Central (abdominal) obesity is a significant contributor to elevated LDL-P, primarily through its effects on insulin resistance and increased VLDL secretion. Even modest weight loss can significantly improve particle number and size. - Reduce Added Sugars and Refined Carbohydrates
Excess dietary sugar, especially fructose, enhances liver fat accumulation and stimulates VLDL overproduction, leading to more small, dense LDL particles. Cutting sugary beverages and processed carbs helps reduce this cascade. - Engage in Regular Physical Activity
Both aerobic (e.g., brisk walking, cycling) and resistance training reduce insulin resistance, improve triglyceride metabolism, and lower LDL-P by decreasing hepatic VLDL production.
Pharmacologic Interventions
When lifestyle changes aren’t enough — or when risk is high — pharmacologic therapy may be necessary. Different agents target various aspects of lipid metabolism:
- Statins
Statins lower LDL-C and LDL-P by upregulating hepatic LDL receptors, but in some patients (particularly those with metabolic syndrome), LDL-P may remain elevated despite reaching LDL-C targets. - Ezetimibe
Ezetimibe inhibits intestinal cholesterol absorption and can modestly reduce LDL-P, especially when added to statins. It’s particularly useful when statin doses need to be minimized. - PCSK9 Inhibitors
These monoclonal antibodies dramatically upregulate LDL receptor recycling, lowering both LDL-C and LDL-P, often into optimal ranges. Particularly effective in familial hypercholesterolemia and high-risk secondary prevention. - Bempedoic Acid
This newer agent inhibits ATP citrate lyase, upstream of HMG-CoA reductase. It lowers LDL-C and LDL-P, with added benefit in statin-intolerant patients. Its anti-inflammatory effect (lowering hsCRP) is also promising. - Fibrates and Omega-3 Fatty Acids (EPA/DHA)
Both target triglyceride-rich lipoproteins. By lowering VLDL, they indirectly reduce LDL-P and shift particles to larger, more buoyant (and less atherogenic) forms. Benefits are more pronounced in patients with hypertriglyceridemia. - Niacin and Pioglitazone
Niacin reduces hepatic VLDL production and LDL-P, but has fallen out of favor due to a lack of outcome benefit in recent trials. Pioglitazone enhances insulin sensitivity and may lower LDL-P levels in individuals with diabetes or prediabetes.
Key Takeaways
-
LDL-P measures the number of cholesterol-carrying particles in the blood and is often a stronger predictor of cardiovascular Risk than LDL-C.
-
Individuals with normal LDL-C can have elevated LDL-P, particularly in the presence of insulin resistance or metabolic syndrome.
-
ApoB provides a similarly robust risk assessment by capturing the total number of atherogenic particles.
-
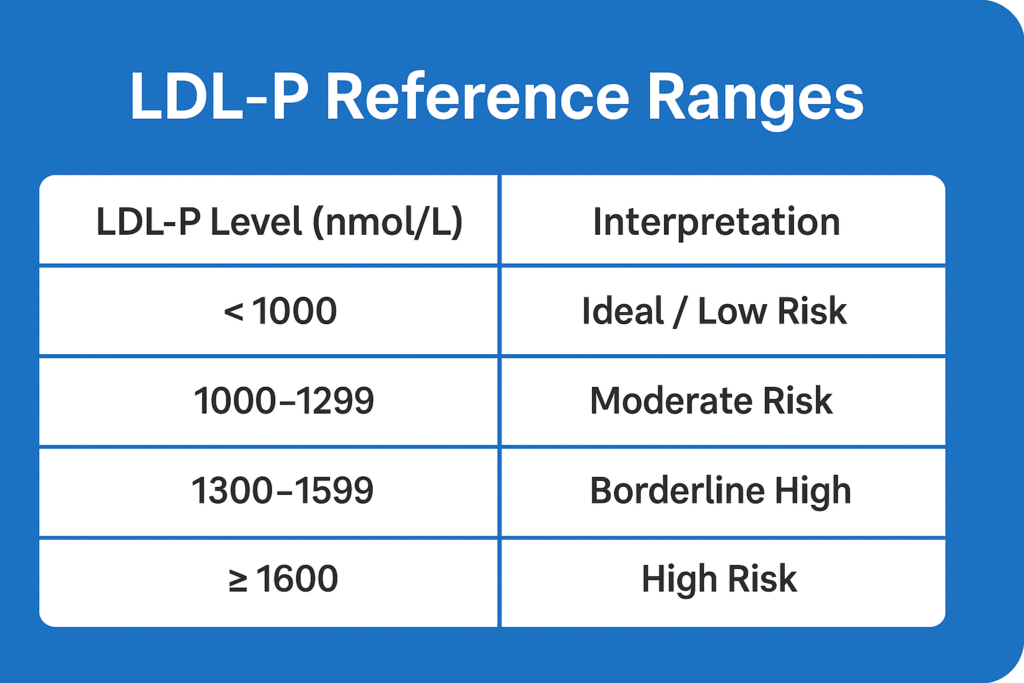
LDL-P is best measured using NMR spectroscopy, with levels ≥1600 nmol/L considered high Risk.
-
Effective strategies to reduce LDL-P include statins, triglyceride-lowering therapies, low-carbohydrate diets, weight loss, and exercise.
Author’s Note:
This article was originally published in 2012 and has been extensively revised and updated in 2025 to reflect the latest scientific understanding of LDL particle number (LDL-P), its relationship to cardiovascular risk, and current clinical strategies for assessment and treatment. As our knowledge of lipidology and atherogenesis has evolved, so too must our approach to interpreting cholesterol markers.
For continuity and transparency, I have preserved all reader comments from the original version. Many of them offer thoughtful insights, personal experiences, and valuable questions that still resonate today.
Related Reading on Doc’s Opinion
- Atherogenic Dyslipidemia (link)
- The Triglyceride/HDL Cholesterol ratio (link)
- When High LDL Leads to Heart Disease — And When It Doesn’t (link)
- The 12-Step Biology of Atherosclerosis (link)
- LDL-C vs. LDL-P: What’s the Difference? (link)
- What’s the Best Lipid Marker to Predict Risk? (link)
- Apolipoprotein B and Heart Disease (link)
- High Triglycerides — And How to Lower Them (link)
- VLDL, Triglycerides & Remnant Cholesterol (link)
- HDL Cholesterol — The Good, the Misunderstood (link)
- 10 Pitfalls of Using LDL-C to Assess Risk (link)
- LDL Particle Number vs. Size — Made Easy (link)
- LDL-P (link)
- Metabolic Syndrome and Insulin Resistance (link)
Sources and Further Reading
- Sniderman AD, Scantlebury T, Cianflone K. Hypertriglyceridemic hyperapob: the unappreciated atherogenic dyslipoproteinemia in type 2 diabetes mellitus. Ann Intern Med. 2001;135(6):447–459. Link
- Otvos JD, Mora S, Shalaurova I, Greenland P, Mackey RH, Goff DC Jr. Clinical implications of discordance between LDL cholesterol and LDL particle number. J Clin Lipidol. 2011;5(2):105–113. Link
- Superko HR, Gadesam RR. Is it LDL particle size or number that correlates with Risk for cardiovascular disease? Curr Atheroscler Rep. 2008;10(5):377–385. Link
- Toth PP, Grabner M, Punekar RS, Quimbo RA, Cziraky MJ, Jacobson TA. Cardiovascular Risk in patients achieving low-density lipoprotein cholesterol and particle targets. Atherosclerosis. 2014 Aug;235(2):585-91. doi: 10.1016/j.atherosclerosis. Link
- Volek, Jeff S., PhD, RD; Phinney, Stephen D., MD, PhD. A New Look at Carbohydrate-Restricted Diets: Separating Fact From Fiction. Nutrition Today 48(2): p. E1-E7, March/April 2013. | DOI: 10.1097/NT.0b013e31828814eb. Link
- Taubes G. Good Calories, Bad Calories: Fats, Carbs, and the Controversial Science of Diet and Health. Anchor Books; 2008.
- Ray KK, Bays HE, Catapano AL, et al. Safety and efficacy of bempedoic acid to reduce LDL cholesterol. N Engl J Med. 2019;380:1022–1032.
https://doi.org/10.1056/NEJMoa1803917. Link - Sabatine MS, Giugliano RP, Keech AC, et al. Evolocumab and clinical outcomes in patients with cardiovascular disease. N Engl J Med. 2017;376:1713–1722. Link
- Jose A. Quesada, Vicente Bertomeu-González, Domingo Orozco et al. The benefits of measuring the size and number of lipoprotein particles for cardiovascular risk prediction: A systematic review and meta-analysis. Clínica e Investigación en Arteriosclerosis, Volume 35, Issue 4, 2023, Pages 165-177. Link
https://doi.org/10.1016/j.amjcard.2022.12.012 - Krauss RM. Lipoprotein subfractions and cardiovascular disease risk. Curr Opin Lipidol. 2010;21(4):305–311. Link
- McNamara JR, Jenner JL, Li Z, Wilson PW, Schaefer EJ. Change in LDL particle size is associated with change in plasma triglyceride concentration. Arterioscler Thromb. 1992 Nov;12(11):1284-90. Link
- Musunuru K. Atherogenic dyslipidemia: cardiovascular Risk and dietary intervention. Lipids. 2010;45(10):907–914. Link
- Wood, Richard J et al. Carbohydrate Restriction Alters Lipoprotein Metabolism by Modifying VLDL, LDL, and HDL Subfraction Distribution and Size in Overweight Men. Journal of Nutrition, Volume 136, Issue 2, 384 – 389. Link
- Mora S, Buring JE, Ridker PM. Discordance of low-density lipoprotein (LDL) cholesterol with alternative LDL-related measures and future coronary events. Circulation. 2014 Feb 4;129(5):553-61. Link
LDL-C and total cholesterol have never been particularly good predictors of who will develop clogged arteries. However, total cholesterol strongly correlates with all cause mortality risk. For example, as total cholesterol rises above 240, there appears to be some increased risk for cardiovascular disease. As total cholesterol drops below 200 there is a steep rise in mortality from infections, parasites, and cancers and increased risk of violent death. https://perfecthealthdiet.com/wp/wp-content/uploads/2011/06/O-Primitivo-Cholesterol.jpg
Unfortunately, last I heard, the American Heart Association was still recommending that total cholesterol be artificially depressed below 200 to decrease risk of heart attack. https://www.theheart.org/article/1371059.do
Yet researchers at Texas A&M university found that higher LDL levels predicted greater gains in muscle mass in a strength training study involving 60 to 69-year-old males. https://www.eurekalert.org/pub_releases/2011-05/tau-cn050511.php
Hopefully, the LDL particle size issue will help exonerate total cholesterol and get saturated fats off the hook for heart disease. https://www.meandmydiabetes.com/2010/03/26/ldl-cholesterol-ron-krauss-md/ After all, saturated fats have very little effect on total cholesterol compared to other dietary factors. https://www.theheart.org/article/1267163.do
Are you seriously trying to imply that low cholesterol causes infections, parasites, cancer, and violent behavior? If you look at that graph, it’s obvious that the countries with low cholesterol are Third World Nations with poor sanitation, disease epidemics, civil war, etc. Do you think you could protect yourself from HIV by eating enough butter, sir?
It’s true. Low cholesterol is bad BAD news. People with high cholesterol live the longest. IN fact for women, really high cholesterol is associated with longevity, but also with increased a little increased risk of heart disease. IMO I think the particles and all that stuff doesn’t mean much either. (I saw only one study on that particle thing and it didn’t convince me) There was a recent study that oxidized LDL is actually the good guy in the process of heart disease. I think heart disease is really an infection in the lining of the artery, and people with high LDL fight the infection a little more agressively so that the plaque ruptures. So IMO they should stop fussing about cholesterol and figure out how the lining of the artery gets damaged and prevent this and prevent the unstable plaque.. BTW I have been unable to effect my LDL cholesterol with diet. the vegetarian diet made it go down a little, cutting saturated fat didn’t do much at all. I would be interested to see if others are able to effect LDL with diet. IMO the body just makes what it makes and it’s not really possible to alter it much. You can make triglycerides go down by cutting sugar and carbohydrates. HDL will go a up a little. HERE you go sir. Low LDL is BAD NEWS. https://www.sciencedaily.com/releases/2012/03/120326113713.htm
butter and diet don’t do much to raise cholesterol. IT’s a myth. I think Sugar does cause a rise in Triglycerides which causes the ratio to get out of wack. I don’t think butter or cholesterol in food does much. I went on Google Scholar and saw that low cholesterol below 150 is associated with all cause mortality everywhere.
genetics plays a big role in cholesterol and triglyceride levels that should not be overlooked. APOE is an important one for efficiency of lipid transport.
Bergamont (Bergamont), in combination with grape seed extract, Bioperine, and Artichoke make for an amazing combination. I take this combination from compoundednutrients.com but you can only get it through a practitioner.
Please expound. What makes it “amazing”? Has it changed your lipid numbers?
I found out 2 days ago I have High Small LDL-P levels 1455 High Triglycerides 160 Low HDL-C 36 Low HDL-P (Total)24.2 High Cholesterol,
Total 210. Im scard to death. Doctor wants to put me on Statin drug. Husband says its hype mother says eat oats. Im afraid of side effects . And afraid of CVD. Im 47 woman . Father died of CVD at age 35 . Mother says it was Lymes disease. I’m afraid to take statin and afraid not to. I dont know what to do. Help please
Hi Jane. Thanks for your post.
A TG/HDL ratio above 4 (in your case 4.6) may sometimes indicate high insulin levels (hyperinsulinemia). I don’t know if you are overweight, but if you are, a low carbohydrate, high fat diet may indeed increase your HDL-C and lower your triglycerides which is probably a good thing. Furthermore, it might improve particle size and particle number.
Your lipid profile in general, with high TG and low HDL, is compatible with the metabolic syndrome. Therefore it is important to know whether you are overweight or not.
Furthermore, it is important to look at your total risk. Do you smoke? Do you have high blood pressure? In Europe, LDL particle number (LDL-P), total, small or large, is seldom used for risk stratification in clinical practice. Your total cholesterol is not very high, I don’t know about your LDL- C.
Personally, I generally I do not recommend statin therapy for this lipid profile alone. However, if your total risk score is high, for example if you smoke, have high blood pressure and prediabetes or diabetes, it can be argued that statins will reduce your risk of CVD.
Finally, let me just repeat that studies have shown that low carb high fat (LCHF) diets may improve a lipid profile like yours, not least if you are overweight or obese.
Saturated fats, in conjunction with adequate supportive nutrition, can lower triglycerides and raise HDL-C. The important thing is to restrict added sugars.
Optimum total cholesterol seems to lie in the 200 to 240 range. https://perfecthealthdiet.com/wp/wp-content/uploads/2011/06/O-Primitivo-Cholesterol.jpg
Thanks for the reply I am 5’3 and 153 # I do smoke.
do you mean unsaturated fats and are you saying no sugar because it turns in carbohydrates. What about omega 3 oats nuts avacado fish oil walnuts fresh fruit vegtables oats . If i eat this diet do you think it will lower ldl-p?
@ Jane Bateman, A person does not necessarily need to eliminate added sugars or omega-6s
from the diet. Just keep them to safe levels. A diet of whole, natural foods such as you listed will naturally limit added sugars and omega-6s without much effort but it may not lower LDL-P.
As for smoking, I suggest you read about the Kitava Study:
https://www.staffanlindeberg.com/TheKitavaStudy.html
https://wholehealthsource.blogspot.com/2008/08/cardiovascular-risk-factors-on-kitava_17.html
My doctor wants to put me on statins because of elevated LDL-P. In May, it was 1578. Now:
LDL-P – 1348
LDL-C = 105
HDL-C = 44
Triglycerides = 73
Cholesterol Total = 164
LDL & HDL Particles
HDL-P (total) = 29.7
Small LDL-P = 513
LDL Size = 21.6
I am 53, never smoked, both parents died from heart disease, I’m 141# (have lost 30 lbs this year). I had bile duct surgery a month ago with elevated liver enzymes and I hate to take medication that will bother my liver. For the last 3 months, I haven’t eaten grains or process foods. The only sugar I eat is fresh fruit. Are statins really necessary in my situation. My doc is more concerned with the LDL-P number and my family history. He feels the family history alone is worth putting me on statins. I don’t have high blood pressure (it was 100/73 today).
Maribeth. Thanks for sharing your thoughts. It would be irresponsible of me to give advice on individual cases. This is certainly a situation where some doctors may want to prescribe statins and some would recommend against it. The decision to prescribe statin therapy in primary prevention is often quite difficult. The clinical guidelines generally recommend looking at total risk, taking into account all risk factors, not only lipids. In your case the total risk is propably rather low, considering that you have never smoked and don´t have hypertension or diabetes. One could certainly wonder, looking at your family history and LDL-P number, whether statin therapy might reduce your risk of cardiovascular disease. However, taking into account the low total risk, your liver enzymes and other possible side effects, I guess many doctors would not recommend statin therapy.
If we reduce carbs in our diet, I think we can assume that food will be replaced with fats and proteins. The additional fats and proteins will increase LDL-C, right? Will it also increase LDL-P? I understand that LDL-P is what we need to be concerned about. Thanks.
Ed. Some studies indicate that low carbohydrate diets may increase LDL-C as you suggest. However, HDL-C seems to increase as well and triglycerides usually go down, which is positive. Furthermore, LDL-particle size appears to increase on low carb, and LDL particle number (LDL-P) decreases. Thus, discordance (between LDL-C and LDL-P) appears to become more prominent.
Hi! I am 36 years old, 5’3, weigh 113lbs. I eat relatively healthy and excerise 6 days a week. I do not smoke. My dad died of congestive heart failure at 53, his identical twin died at 46 from a massive heart attack and their dad died at 53 from heart disease. All 3 smoked. Dad had his first heart at 37. I just had extensive blood work done and here are the results. My doctor wants me to take a baby aspirin daily and retest in 3 months. I would love your thoughts on this. I am not sure about taking the baby aspirin daily.
HDL: 97
LDL: 103
Triglycerides:59
total Cholesterol:97
LDL-P: 1101
APO B: 82
APO A-1: 181
I have a ton of other numbers. Please let me know if you need to see all of them 🙂 Thank you so much!
Krstina. I understand your family history is a cause for concern. Remember however that your dad, his brother and your grandad were all smoking males. You being a nonsmoking woman is quite different. The regular exercise, and I am assuming a normal blood pressure is also positive when assessing your total risk. I think your lipid numbers are indeed quite good as well, apart from the LDL-P. The goal for LDL-p is less than 1.000. 1300-1600 is generally considered moderate risk and above 1600 is high risk. However considering that all other measures are very good, I don´t think you need to worry that much. Apo B and Apo A-1 values are fine. Total cholesterol (assuming the number is 197), LDL-C, HDL-C and triglycerides are all quite good numbers. TG/HDLratio is also low which is positive.
If we use the traditional algorithms, your total risk is indeed very low, despite the family history. I am not aware of any scientific studies showing a clear positive effect of baby aspirin under similar circumstances, which is the reason why I would not prescribe it if you were my patient. I do not think it will affect your lipid numbers. I would not give a cholesterol lowering drug either under these circumstances. Continuing the healthy lifestyle, healthy eating and exercise, definitively, in my opinion is the best thing you can do.
Thanks for the post.
Thank you do much for your quick response! The total cholesterol is 206. ( 3 little ones running circles around me while typing). Also, my Lp-PLA2 is 236. This has to do with inflammation? What are your thoughts regarding that number? I am told this is a high risk number for me. Thank you do much!
Kristina. There is still some uncertainty about the value of Lp-PLA2 measurements. There seems to be a positive association between Lp-PLA2 levels and vascular and nonvascular outcomes in many studies, but these are observational studies and can´t establish causality. https://www.theheart.org/article/1071965.do
High sensitivity CRP (hs-CRP) is probably the most commonly used marker of inflammation. Some studies have raised the possibility that hs-CRP could be used to target high-risk patients who may benefit from statin use. https://ukpmc.ac.uk/abstract/MED/16442935
I just had my labs done due to feeling fatigued and tired all the time as well as headaches. My LDL-P was 2051, LDL-C 131, Triglycerides 147, Cholesterol 212. My small LDL-P is 787. Also, my LP-IR score is 50. I am so confused about all the information about diets and the fact that my LP-IR is high. Now I’m confused about diabetes and insulin resistance. I am overweight, 185 and 5’2″. My Vit D is also low at 27.1. I know I need to maintain a diet and decrease weight, but the proper diet, what to eat and what not to eat, is totally confusing to me. Looking for suggestions! Thanks so much!
Rebecca. Please discuss your symptoms and lab results with your doctor and get his advice.
What concerns me with your lab results is the elevated LDL-P and small LDL-P. Triglycverides are also borderline high. Total cholesterol and LDL-C are not that bad numbers. Your BMI is 33.8. Your LP-IR certainly indicates some insulin resistance.
Lipid problems, including higher triglycerides, decreased HDL levels, and increased small, dense LDL particles, have been shown to be atherogenic. In obesity, these lipid disorders seem to be closely related to insulin resistance. Weight loss and exercise, even if they do not result in normalization of body weight, can improve lipid profile and thus reduce the risk of heart disease. Therefore, weight loss is extremely important. https://www.ncbi.nlm.nih.gov/pubmed/14711065?dopt=Abstract
Furthermore, evidence suggests that carbohydrate restriction, positively influences the aforementioned lipid problems. https://www.nutritionandmetabolism.com/content/3/1/24#B1.
So, for an individual with obesity, insulin resistance, elevated LDL-P and triglycerides, carbohydrate restriction is certainly something I would suggest. It usually helps inducing weight loss and will likely improve lipid profile.
I went LCHF Paleo in 2011 and my cholesterol numbers have worsened considerably. I am worried that I might have familial hypercholesterolemia.
I am a 49 year old female, non-smoker, low-normal blood pressure, low (but treated) thyroid, BMI of 23.
Now (pre-Paleo)
Total Chol. 298 (195)
LDL-C 136 (98)
HDL-C 134 (85)
VLDL 28 (9)
Trigl. 140 (61)
CRP 0.9 (1.6)
My doctor wants to prescribe statins and is unwilling to order an NMR (I’m in Massachusetts where it is illegal to get any blood tests without a doctor’s order – even online). I think I can, however, drive out of state for a heart (calcium) scan which I can schedule myself. If the heart scan is good, should I still try to find a way to get the NMR? Many thanks!
Thanks for the post Dottie. I find your experience interesting. It surprises me a little bit that your Total Chol and LDL-C have gone up this much. It surprises me even more that your TG have gone up as well, which is uncommon on Paleo and other low carbohydrate diets. However, your HDL-C has gone up considerably which is very positive. Therefore, your TG/HDL-C ratio has only gone up a little bit. I see from the numbers that your LDL-C is calculated (not measured) using the Friedewald equation, but it should be reliable anyway in your case.
There appears to be some inconsistency in how a Paleo type diets affects blood lipids. In one study this type of diet appeared to lower Total Chol and LDL-C as well as TG. https://naturetherapies.com.au/wp-content/uploads/2012/04/Paleo-diet-Study-Frssseto09.pdf
In another study a Paloelithic diet appeared to elevate LDL-cholesterol in diabetic individuals.https://www.biomedcentral.com/content/pdf/1475-2840-8-35.pdf
Clinical experience and individual reports indicate that elevation of Total Chol and LDL-cholesterol is not uncommon on a Paleolithic Diet. However, HDL-cholesterol seems to rise as well and triglycerides usually drop. Many of the Paleo followers believe that the elevation of Total Chol and LDL-C is nothing to worry about because they consider cholesterol in itself not dangerous and they don´t believe it is a causative factor in cardiovascular disease. However, I don´t think there is available evidence for us to believe that. There is so much evidence indicating that LDL-C is associated with cardiovascular risk. However, maybe an elevation of HDL and a drop in TG on Paleo, might counteract the effects of elevation of LDL-cholesterol. It appears that the TG/HDL-C ratio is an important predictor of risk. This ratio is highly associated with insulin resistance. In your case this ratio is just above one (on Paleo) which is relatively low. A cutoff of 3.5 has been suggested to identify patients at most risk for cardiovascular disease.
Although your LDL-C has gone up on Paleo, it is possible that your LDL-P has not (discordance). That is what an NMR might reveal.
Your CRP has gone down which is generally considered positive.
I doubt that you have familial hypercholesterolemia (FH), considering your Total Chol and LDL-C before Paleo.
These are the main symptoms of FH:
•High levels of total cholesterol and LDL cholesterol.
•A strong family history of high levels of total and LDL cholesterol and/or early heart attack.
•Elevated and therapy-resistant levels of LDL in either or both parents.
•Xanthomas (waxy deposits of cholesterol in the skin or tendons).
•Xanthelasmas (cholesterol deposits in the eyelids).
•Corneal arcus (cholesterol deposit around the cornea of the eye).
Personally I am usually a bit conservative when prescribing statins in primary prevention. I do not only look at the lipids. I usually look at other risk factors as well such as familiy history, smoking, blood pressure, diabetes etc. Of course, if you have FH, you should have statin treatment.
I also wonder what your diet was before Paleo and why you decided to change…
Hello Doc, I have been watching your video and reading your articles, and I just received my results from an NMR and VAP cholesterol test. Below are my NMR results and I am very concerned and hoping you can give me some advice for area of my diet and exercise to explore.
My results:
LDL-C 217
HDL 68
VLDL 16
Cholesterol Total – 301
Trigs 66
LDL+VLDL 233
LDL-R (Real) 190
Lp(a) 16
LDL-P 1812
LDL Density Pattern: A
I weigh 170 lbs, 5’10”, male. My diet is generally low carb, low grains. I eat eggs, steak, chicken a few times per week each. Not much milk and I exercise 5-6 times per week, which includes 3-4x weights, 4-5x cardio.
Any thoughts? Thank you!
Hi Dave. As you probably know genetic factors highly influence our blood lipid pattern. I presume you have a family history of high cholesterol, correct me if I am wrong. You seem to live a healthy lifestyle, BMI is normal, lots of exercise and a relatively healthy diet.
Total Chol and LDL-C are quite high and so is LDL-P. The positives are a relatively high HDL for a male and relatively low levels of TG. TG/HDL-C is close to 1 which is fine. LDL density Pattern A suggests that large particles dominate which is positive. Lp (a) is not that bad.
It is very often hard to predict how diet affects our lipid pattern and there is a lot of individual variation. I would certainly be curious to know whether you could lower your LDL-C and LDL-P by cutting down on the consumption of cholesterol and saturated fat, as indeed recommended by the American Heart Association and the European Society of Cardiology. You could even choose a Mediterranean style diet, or DASH, increasing the consumption of whole corn, fish, olive oil and eat lots of vegetables and fruit.
Considering your BMI and lipid pattern, there are no signs of the metabolic syndrome. Therefore you probably don´t have any insulin resistance and no carbohydrate intolerance. So, in my mind there is no need for you to avoid healthy carbohydrates and starchy food unless you prefer to do so yourself. However, by all means, stay away from simple refined sugars and junk food.
I guess many doctors will suggest statin therapy when looking at your lipid pattern. Many specialists consider an LDL-C level above 190 to be a clear indication for drug therapy, no matter what else you find. This decision may however have to take into account your age, previous disease history ( I am indeed assuming you are healthy) family history and other risk factors.
Good luck Dave. Will be happy to hear about your progress.
Thank you, Doc, for your comment. Yes, I am healthy, have no risk factors and do not have a history of high cholesterol in my family. I am going to take your advice and add carbs to my diet, probably sweet potatoes and white rice, and more nuts, and then retest in a month, unless you think this is not enough time.
Also, I was wondering what your thoughts are on low-carb eating and the effect of T3 or rT3. Could low thyroid function be the cause of high LDL-P? I was considering getting tested for thyroid function and testosterone if I test in one month. Thoughts?
Thank you for your help.
Low thyroid function has been associated with elevated levels of blood cholesterol. Thyroid hormones seem to be involved in LDL and HDL metabolism, although the mechanisms are still a bit unclear. I agree that you should have your thyroid function tested. There is a recent publication indicating that hypothyroidism (TSH levels over 10 mIU/l) is associated with a significant reduction in LDL particle size and a higher prevalence of atherogenic pattern B. https://www.ncbi.nlm.nih.gov/pubmed/23039873
One month may be a little to short to evaluate the effects of diet changes on blood lipids, but you might see some trend. I often recommend reevaluation in six months following a change in lifestyle and/or dietary habits.
Thanks, Doc. As it is easy to overdo these tests, which test do you recommend for Thyroid?
Here is a site I have been using: https://www.accesalabs.com/thyroid
Thanks.
Measuring TSH is usually enough to test for hypothyroidism (low thyroid function). If hypothyroidism is present, TSH will be elevated. If hyperthyroidism (overactivity of the thyroid gland) is suspected Free T4 is ofte measured as well. Other tests are seldom needed.
Yet, my wife is hypothyroid and despite taking 100mg of T4 daily, she still has symptoms such as brittle nails, hair loss, insomnia. After reading Sarah Gottfried’s book, the Hormone Cure, she had her free T3, free T4, reverse T3 and antibodies tested to determine if she had Hashimoto’s, which it looks like she most likely has. Most articles she has read would indicate that TSH alone doesn’t tell you squat and that the other tests are vital. I suspect she is a candidate for Armour, although her doctors are reluctant to prescribe “natural” products and have so far started her on Cytomel in addition to her Levoxyl. Too soon to see what effect that is having.
Thank you, Doc, for your informative reply. Regarding FH, I tend to agree that it would likely have shown up earlier in life. Prior to Paleo, I had been on a SAD/ Weight Watchers diet for 10 years. My diet was chronically calorie-restricted, VLF, and nutrient sparse (I believe that may have caused the hypothyroid). I have read that FH can be hidden by a low-fat diet, so, I am going to find a way to get an NMR.
On a positive note, I’ve just learned from 23andme that I don’t carry the ApoE ε4 variant. So, I’m now thinking the low thyroid function may be the cause of the high LDL and TG (that darn TG really should have gone down on VLC!). Thus, I wonder if the VLC diet is suppressing my thyroid and thus interfering with cholesterol metabolism… (ah, so many variables). I wish my GP knew as much as I do about this. Better yet, I wish more doctors were as up on the research as you. Anyway, if it would be of interest to you or your readers, I’ll post again once/if I figure it out.
Thanks for sharing your thoughts Dottie. I will be very happy to hear about your progress.
Just came across this site. I too have experienced the increase of TC and LDL. However as I consider the FH diagnosis, everything Ive read is that FH is almost never been able to be controlled by diet alone, which clearly is not the case in many Paleo eaters that encounter this sudden rise in TC and LDL.
Hi Doc! Went to the doc yesterday to talk about Cholesterol & labs and got scared out of mind!! Here are the results of my labs:
Total Chol-209
LDL-C-148
HDL-C-37
TRIGLYCERIDES-60
NON HDL C-172
APO B-128
LDL-P-2430
LP MASS-20
HS-CRP-25.7
I am overweight but I am dieting right now and have been successfully for about a month. I have lost 13 lbs since these labs were drawn. At the same time these labs were drawn I was also being checked for a UTI that did come up positive. Was wondering if the UTI caused the high hs-CRP? I am 33 yrs old, I do smoke and now weigh 187 down from 199. My blood pressure is normal now because of the weight loss and my doc said I would probably get to come off of my bp meds sooner than later because the weight loss seems to be bringing it down. At least I got some good news. Also, heart disease runs in my family through my grandparents. My doc wants to put me on Lipitor and Niaspan 500 mg & 1 coated asprin a day. Mixed advise given to me about Statins and Niacin. Would like to know what you think. Confused and scared I am going to drop dead from a heart attack at anytime. Thank you and any info would be greatly appreciated!!! Amanda
@ Amanada. UTI can definitively raise hs-CRP. Measuring hs-CRP when you have an active infection can therefore be misleading. There appears to be a lot you can do to reduce your risk for heart disease. Quitting smoking is extremely important. If you continue losing weight, your LDL-P and APO B will probably improve. You may have insulin resistance so limiting sugar and carbohydrates might be helpful. I think you should discuss with your doctor the possible advantages and disadvantages of medical therapy.
I am 31 yr old female. I weigh 120 lb and am 5’3 inches. I eat relatively healthy, including whole grains, fruits, vegetables, lean meats, and dairy into my diet. I don’t eat a lot of fat, but when I do I try to use healthy fats like olive oil or Smart Balance spread which is supposed to help maintain healthy cholesterol. I usually don’t eat a lot of junk, but I would usually bake something sweet about twice a month. My doctor did a full array of blood tests for me in February, where I had some parts of my cholesterol that were too high. I kind of thought it was a fluke, so didn’t think too much about it until I got retested this month. My LDL-P is 2153, My LDL-C is 125, My HDL-C is 47, my Triglycerides are 144, My total Cholesterol is 201, My small LDL-P is 1575, and my LP-IR score is 55. I was pretty surprised when my doctor stressed how poor my scores were since I do traditionally abstain from junk, I don’t smoke or drink, I’m not over 50, and I’m not overweight. Though my parents and grandparents have not died of heart disease I have learned that one of my grandmas had heart problems and that her brothers died of heart attacks, both after shortly being told by a doctor they looked healthy.
I would like some advice how to get my numbers to look better. I’ve started working out more vigorously than before (though I was never sedantary) and I’ve eliminated sweets (definitely starting to miss the baking), and I’m taking niacin daily. What else can I do? My doctor mentioned that if my blood work in February doesn’t look better she would consider putting me on medication. I really feel too young to be taking cholesterol meds.
@ Katie. This is a difficult situation as you seem to eat healthy, have no overweight and do a lot of exercise. Your genetic predisposition does not appear strong either. The TG/LDL ratio and the LP-IR score may indicate you have some insulin resistance. LDL-P and small LDL-P are high as you are aware of. If you look into the scientific literature, a low carb high fat diet is probably more likely than a low fat diet to raise your HDL and lower your TG, LDLP and small LDL-P.
I am told that LDL-P and ApoB measure the same thing. But how do the numbers translate. I don’t have a LDL-P number. I have 184 ApoB which the report says is high risk. But I see people posting LDL-P numbers in the 1000’s and 2000’s. What does a 184 ApoB translate to in LDL-P?
Joe
You can’t directly translate ApoB to LDL-P. There is a strong correlation between ApoB and LDL-P which means that when ApoB is low, LDL-P tends to be low as well and when ApoB is high, LDL-P tends to be high.. However, sometimes there is discordance between ApoB and LDL-P. Thaht could mean a relatively high LDL-P despite a relatively low ApoB.
So it’s not always simple.
Don’t know whether you have access t this paper here but you may be able to see the abstract.
Doc, are there any innocent, non-dangerous conditions that can cause a spike in inflammation markers? I always had low crp. Went on a high fat/low carb diet a few years ago and my LDL went to 300. My crp was 2.4, a little higher than in the past (used to ranged from 0.3 to 2.0). I decided to go low fat for a month and recheck. My LDL went down to 120 but my crp went from 2.4 to 12.3. fribrimogen from 380 to 507 and LpPLA2 from 228 to 266.
I had given up coffee and was having slight withdraw, and had swollen glands in the neck and a slight cold.
Joe
There are a number of factors that can elevate hs-CRP and other markers of inflammation. Infection is one of them. So if you had a cold and swollen glands, that may surely have played a role.
https://www.docsopinion.com/health-and-nutrition/hscrp/
Do any of these tests directly measure inflammation on the wall of the artery, or do they all just measure general inflammation? And if its just general inflammation, is it the case where elevated inflammation levels as measured by these tests (CRP, frbrimogen, LpPLA2) is only a problem if the inflammation detected happens to be from damage in the inside of the arteries that are inflamed, or does inflammation from other parts of the body (arthritis etc) cause damage to the arteries and raise risk of CVD?
Joe
Measurements of these markers reflects general inflammatory activity. We can’t differentiate between inflammation within the cardiovascular system or elsewhere in the body.
The other question is more difficult to answer. We know that people with some inflammatory disorders such as rheumatoid arthritis are at increased risk of cardiovascular disease suggesting that the inflammatory activity associated with these disorders may negatively affect the cardiovascular system.
So for someone to have ‘chronic inflammation’ those markers should be up all time? I have been trying to figure out why my inflammation went from low to med to sky high.
I recently switched from a combo of traditional lifting and cardio to less frequent, shorter but more intense workouts. Part of that is ‘super-slow reps’. The negative, or eccentric part of the lift, lowering it, has long been claimed to cause more micro damage to the muscle. Doug McGuff says now that the concentric part of the lift done very slowly does even more ‘damage’. Usually it is done fast. This is said in a positive way; the more damage, the stronger the muscle gets when recovered – and the longer it takes – so the more time off.
My point is that since I started this, I got rosacea on my nose, and higher inflammation – although I have been on it for a year, at which time the rosacea started, but the inflammation seems to have just spiked sky high recently
Think its possible that these slow reps, to failure and beyond (isometric pushing after failure) could be causing more muscle damage and raising inflammation? I’ve done very hard, excessive, crazy workouts before, but never these slow reps to failure and beyond.
I’ve been a superslow guy for almost 20 years and am intrigued by this question.. especially b/c I’m doing it pretty intensely and now 3x/week up from previously 1x/week. My LDL-C and LDL-P is really high so would be interested in any possible correlation here as well.
Hi Doc! I’ve just got my results, and I’m a little concerned with the numbers. I never smoked, drink only socially, don’t exercise, love sweets (ice cream, chocolate, cakes, etc), a little overweight, but accumulate fat basically in my stomach. My energy levels change, my sleep pattern is crazy. Please, help me to figure out what I need to do. Today I tried not to eat sweet and I must tell you. It’s hard. My mouth waters when I see it, and I get a little upset because of that. AST(SGOT) high – 49; ALT (SGPT) high – 74; Vitamin D, 25-Hydroxy low – 16.9; LDL-P high – 2123; LDL-C high – 107; Triglycerides (high) – 211; Small LDL-P (high) – 1317; LDL size (low) – 20.3; LP-IR Score (high) 79. I don’t have any family history. I’d prefer not taking drugs if it’s all possible.
Hi Marcia. The liver enzymes, AST (GOT) and ALT (GPT) are only marginally elevated. There appears do be a typical discordance between LDL-C and LDL-P; LDL-C is not that bad, but LDL-P is high. Triglycerides are high, so is small LDL-P. LP-IR score is elevated suggesting insulin resistance. This is a lipid profile you would expect to see in an individual with the metabolic syndrome.
I would focus on two things, both important.
1) Try as much as you can to stop gaining weight. I know it sounds easy, but I have to emphasize it. I don´t know about your age: you look young in the picture by the way. Sometimes weight gain occurs very easily over a short time, so stay alert.
2) I hate to tell you this, but I think it is very important for you to avoid sugars. I know it can be though, but I know that you know how important it is. I´m not necessarily suggesting that you avoid carbs altogether, but definitively sugar. Maybe you should study glycemic index (GI) and select carbs with a low GI. Have you studied the GI-diet which is quite popular these days?
Good luck and thanks for the post.
I am an almost 63 year old female, low blood pressure, get lots of exercise (walk almost every day at least 4-5+ miles and do Pilates 2-4+ times/week), eat a mostly plant –based diet w/lots of greens, onions, garlic, mushrooms, raw nuts, some fruit, etc. plus wild Alaska salmon almost every day. (Started eating fish regularly when I started taking my ldl seriously around June of this year.) Take one fish oil tablet usually every day (EPA 360mg/DHA 240 mg). I am about 5’ 1” and weigh about 116. (Have been bringing down my weight by strictly eating a high-density diet.) My mother had congestive heart failure, but smoked and took terrible care of herself. My father, born in 1925, had a mild heart attack, but has taken such good care of himself that 15-20 years post-bypass his arteries are free and clear. (He does take statins.) He smoked until he was about 35, I believe.
I took an exercise stress test and was told I performed at an active 23-25 year old level.
When a cardiologist saw that my ldl was 196, he said that based on my family history, he didn’t think I could bring it down with diet, so he wanted to put me on statins. That made me mad so I set about doing just that. After the first 6 weeks I brought it down to 160. After another 6 weeks to 129. But then it crept up to 147 and then basically stayed there the next time. I was eating dark chocolate with caramel, however, plus other chocolate during this time.
I had gestational diabetes (in 1986), but have avoided diabetes. I may qualify as having pre-diabetes, however. I do try to include protein whenever I eat, but am not as good about this as I should be.
My hs-CRP was last 0.05 on a 0.00-0.30 scale and has been around that for quite some time.
My last two lipid studies were as follows (the most recent one first):
Cholesterol 243 244
Triglycerides 109 87
HDL 55 62
LDL, direct 146 147
The really scary part, though, is my LDL-P = 2301.
Other results follow (taken the same day that my cholesterol was measured at 160 at another lab):
LDL-C 176
HDL-C 58
HDL-P (total) 35.2
Small LDL-P 778
LDL size 21.6
Large VLDL-P <0.7
Large HDL-P 5.6
HDL size 8.8
LP-IR score 26 (fasting)
I have probably left out something important, but imagine you will ask.
Hi Sandy. Your BMI, blood pressure, lots of exercise, no-smoking certainly indicates you are taking good care of your self. You do have family history of CAD and your blood lipids have caused some concern. However, considering the usual algoritms, your total risk is probably not very high. LP-IR score indicates no insulin resistance. Most doctors recommend statins if LDL-C is above 190, so I understand your doctor very well when he recommended drug therapy, when your LDL-C was >190. However, you managed to lower your LDL-C which is great. The high LDL-P worries me a little bit. You can argue for and against drug therapy in your case but the effect of statin treatment in primary prevention, if total risk is low, is quite small.
There are two options.
1) Continue taking good care of yourself, exercise and eat healthy. Have your lipids tested again in 6-12 months.
2) Start statin therapy which will probably lower both your LDL-C and LDL-P signficantly. However, there is always a possibility of side effects although these drugs are generally well tolerated.
If you ask 100 cardiologsits which way to go, 50 percent will probably say 1) and 50 percent will say 2). So, there is really no right answer, there is no truth. If you are properly informed you might even want to make this decision yourself. I would probably go for number 1).
PS I forgot to mention (at least) a few things. First, I very much want to avoid taking drugs, if at all possible, and have the discipline to do what is necessary, I believe, assuming it can be done. Second, I have Hashimoto’s, which last time measured at 1204. And, for what it’s worth, I have acquired angioedema triggered by NSAIDs.
Hi Doc,
I am 51 6’2 203lb male. I was diagnosed with celiac disease 2 years ago and soon after my weight went
up to 220 after plummeting to 190. Blood Pressure was controlled by norvasc 5mg and cardiologist insisted on taking simvastatin, to which I have resisted until now. Father and both grandfathers died from heart attacks. Mother’s side has history of diabetes and high cholesterol.
NMR profile:
LDL-P 2333
LDL-C 163
HDL-C 35
triglycerides: 116
Total Cholesterol: 220
HDL-P 23.2
Small LDL-P 1561
LDL size 20.1
LP-IR score 64
I do moderate cardio exercise with weight training. I try to stay low carb as much as possible but have a major weakness for potato chips which I usually can resist. I mostly eat mixed greens, chicken, vegetables, and nuts.
I only drink milk with coffee. I am going back on bp meds as my pressure started to creep up again after a nice hiatus from having to take them. any words of advice would help. I
Hi John. Thanks for the post. The high LDL-P certainly put you at higher risk. Considering your BMI and LP-IR score it is likely that you have insulin resistance. Losing weight is very important in this situation. I definitively agree that carbohydrate restriction is sensible. Under these circumstances, considering the lipoprofile, high blood pressure and family history of coronary artery disease, I usually recommend statin therapy unless there are contraindications for such treatment.
Dear Dr. Sigurdsson, I am a 71 yr. old male and have been lucky not to have hight blood pressure, and no Diabetes,but both of my parents did have it. I have total body weight of 146 lbs. On my recent visit to my Dr. My test Total cholesterol is 170. Triglycerides 55, Hdl 68, Ldl (direct)82, and vldl 11, also HDL risk factor is 2.5, which is low. Fasting Glucose is 91 and Hemoglobin A1C is 5.6 four months ago but as of this new test date is 5.9. The cause for my question to you is that I have had in the past a up and down results for this one test named LDL-P which now is at 1087. back in 2010 it was 1036, and in 2011 it was 1030, and in 2011 it was 1009, and in April of this year it was 1006. This most current test is dated 11-16-2012 and is 1087. also the result for LDL size is 21.1. My Dr. who I dearly respect wants me to take Creastor 5mg. 3 times a week to get this number down. Honestly I do not want to take this Med. I would like to try whatever for the next three months before he re tests my blood. I do not smoke as I quit that over 40 years ago. I drink 2 bottles of beer a week and do drink any hard suff at all. Maybe a glass of red wine on the weekend at dinner. All of theses Tests are done buy NMR Lipo Profile. Test for the Lab known as Health Diagnostic Labs Inc. This LDL-P Particle size test shows that I may have of I am prone to have atery problems as well as plack problems ???. It is enough to make me crazy. Not to put you on the spot as I have read some of your comments to other Posts could you give me your thoughts. God Bless you for your caring as you do about us Folks. And happy Holidays to you and Yours.
@ Anthony. Thank you for your post and all the kind words.
As you know I do have to be careful when it comes to individual recommendations. Your doctor will surely know much better than I what´s best for you. I can only reflect on what you have written in very general terms. In general, your risk profile appears to be low; no smoking, no hypertension, no obesity, no diabetes. There is family history of hight blood pressure and diabetes but no history, as it appears on premature coronary events. Your general lipid profile does not cause much concern, total cholesterol and LDL-cholesterol are not elevated. LDL-P repeatedly just above 1000 which is not all that bad. For a low or moderate risk individual an LDL-P less than 1300 is considered optimal.
In my opinion a lipid profile like yours does not cause that much concern. Furthermore, your total risk appears low. Considering that you have no previous history of cardiovascular events, statin therapy certainly might sound a little aggressive. However, I certainly don´t know all the details of your history. Ask your doctor why he considers your risk to be high and ask him to explain why he wants to put you on statin therapy. There may be reasons that I´m not aware of.
Dear Doctor, Its Anthony again and a sincere Thank you for your response. What I will do is not take the Creastor as My Dr. suggested , but I will excirse more , Walk more and stop eating Cheese, and Potato chips that I adore. I have read and read about diets , and a question I ask you now is what diet helps to lower LDL-p and is the most Heart Healthy diet to live by. I eat chicken, fish, and red meat only once a week. I do drink 4 cups of coffee in the am with oat meal and bannans. 5 prunes, and 3 tablespoons of blueberries in the hot oat meal with shim milk fat free. Ice Cream 1x per week. Is it what I am eating that makes the ldl-p numbers seen high as My doctor said the new target numbers are at 750 now not 1300, as the testing Lab says is opitmal. What I am trying to do is really to live as healthy as my Grandmother who made it to 97. Her Mother made it to 103. and would you believe her sister made it to 105 years old. That is some track record, but they all lived in different times. By the way I am a hyper person and I have a Person type you would call the ” A ” type. If their is any book written about the diets that help to keep this LDL-p in check please advise and any further comment from you is so much appreciated. Gratefully Yours. Anthony
Greetings Doc – I have studied your previous responses but am still confused about my direction.
I am 43, male, 5 ft. 10 in., non smoker, normal blood pressure and light exerciser (walking about 3 times per week). No family heart problems in the past.
I started a Paleolithic diet after a lipid profile I received last year.
I also began supplementation as follows:
Vitamin D at 3000 IU daily (2011: 21.2 ng/mL 2012: 66.6 ng/mL)
FISH OIL at about 2 grams daily
Here’s the before and after:
PRE- PALEO November 2011
1784 LDL-P
115 LDL-C
54 HDL-C
315 Triglycerides
232 Cholesterol, Total
31,9 HDL-P (Total)
971 Small LDL-P
21.1 LDL Size
83 LP-IR Score
185 Weight
POST – PALEO November 2012
2272 LDL-P
199 LDL-C
57 HDL-C
93 Triglycerides
275 Cholesterol, Total
35.6 HDL-P (Total)
639 Small LDL-P
21.6 LDL Size
31 LP-IR Score
168 Weight
I basically cut out 80% of my carbs by avoiding wheat and sugar as much as possible.
I still eat them sometimes (pizza and ice cream on weekends). I eat eggs everyday for breakfast.
So I improved in certain areas and reduced my insulin resistance, but did I increase my risk for heart problems?
Might a further reduction in carbs make a difference? DOes high dose fish oil affect the results?
I suspect it is all interrelated but I’m concerned about such a high LDL-P.
Thanks so much for your efforts on this website. Your opinion is greatly appreciated!
Thank´s for the post Charles. I understand your confusion. Your lipid profiles pre – and post Paleo show very well how difficult it is to predict how our lipid numbers react to different diets. The fact that your total cholesterol (TC) and LDL-cholesterol (LDL-C) go up on Paleo is not surprising. Generally, carbohydrate restriction with increased consumption of fat elevates TC and LDL-C. However, more than 50 percent elevation of LDL-C on Paleo is more than I usually see.
The lowering of TG and insulin resistance (LP-IR score) is something you would expect on Paleo. However, I would have expected HDL-C to rise a little bit more. Indeed HDL-P goes up a little bit.
Generally, cholesterol rich foods, like eggs don´t elevate TC and LDL-C very much. However, studies have shown and I have also seen in my practice, that a small percentage of people who eat a lot of eggs elevate their TC and LDL-C quite much although this is not the general rule. Maybe you are just one of those individuals. However, it surprises me a bit that LDL-P goes up at the same time as the number of small LDL-P decreases. The Paleo theoretics might say to you: “Don´t worry about TC and LDL-C, it is all about LDL-particle size. You have a lot of large particles and should not have to worry”.
I have seen a lipid response like yours a few times among people on low carb high fat diets. I am not ready to ignore LDL-C as a risk factor. Clinical guidelines recommend LDL-C as the main target for treatment with lipid lowering drugs. An LDL-C above 190 is something that most cardiologists want to treat with a statin drug, no matter what. Remember that your LDL-P is also very high. When I see a lipid response like yours I always recommend my patients to reduce the consumption of cholesterol and saturated fat. This involves eating less eggs and animal and less dairy fat. I usually urge them to eat mono-and unsaturated fats including fish oils and Omega-3. In my opinion a Mediterranean type diet is very sensible under these circumstances.
Wish you all the best.
My personal anecdotal experience — starting as a prototypical metabolic syndrome case whose good numbers were all low and whose bad numbers were all high: Eating low-carb high-fat paleo significantly reduced my triglycerides and raised my HDL; and then going on a statin and naicin massively brought down the TC, LDL-C, and LDL-P. Those two approaches seem to be working great for me.
I didn’t get a lipid profile done just prior to converting to a LCHF diet early this year (unfortunately!). Hadn’t had cholesterol checked in a couple years — so I can’t say for sure exactly what the diet alone did. 6 months into the diet, and not under influence of drugs yet, I tested TC 280, LDL 190, and LDL-P at over 2800! That’s pretty bad. But the good was that my HDL had increased to 40 (from 32 two years ago) and TG was down to 180 (from nearly 500 two years ago … even 20 years ago in my mid-20s, I had tested in the 300s on TG).
So my Doc put me on simvastatin and Niaspan. He advised that low-carb was OK but I should minimize red meat and saturated fat (ie, a low-carb Mediterranean or South Beach kind of diet). I took the drugs and ignored his diet advice, kept eating all the bacon, eggs, cheese, and beef I wanted, with whipping cream in my coffee, all 5 cups a day. After 4 months on the drugs, I’ve just tested at … TC 126, LDL-C 52, LDL-P about 1280. HDL up to 45 and TG down to 140. I clearly remain a met syn case, hence still have somewhat high TGs and LDL-P that’s above ideal (though better than 50th percentile I do believe). But have to say the drugs clearly had quite an impact. I personally suspect that if I did anything other than a low-carb high fat diet my triglycerides would explode again, and probably the LDL-P along with it.
Dr Sigurdsson,
I would like to start by saying that I just came across your website and have been quite impressed. I too am one of those people on “lowish” carb Paleo with elevated LDL-C/P. It is quite difficult to find good data that combines the principles of a low carb approach to looking at lipids(i.e. high HDL, LDL size, low TG/HDL ratios) and the reality of LDL particle numbers. Some of the comments you have made above have been quite insightful and on the money. As a physician (anesthesiologist) I appreciate that. In my personal lipid situation I have spoken with many physicians and frankly the majority had never even heard of LDL-P. The recommendations I have received are quite varied and often just based on LDL-C number.
From my reading of low carb and Paleo blogs, I believe my situation is fairly common and we all could use your insight. I would truly love to hear your opinion on my situation. I am not asking for specific medical recommendations but more of a way to look at the situation or any suggestions about specific reading.
My father and paternal grandfather were diagnosed with coronary disease in their mid 60’s. In 2003 (age 40) I had a cholesterol of 220 and an LDL 160. I was started me on simvastatin initially at 10 or 20 mg but ultimately up to 40mg/day.
Date (Total Cholesterol/HDL/LDL/TG)
2003 Statins started
2004 140/63/61/79
04/2009: started to decrease processed carbohydrates
10/2009 166/72/82/44
07/2010: started low carbohydrate “Paleo” diet, higher in saturated fat, with no wheat minimal grains and no seed oils.
12/2010 218/98/93/53
Calcium Score Obtained (result: zero) Statins stopped due to side effects (libido, muscle soreness(mild), multiple colds and memory issues(per wife)).
05/2011 278/93/170/80
Anyway since stopping the statins I feel great. I have repeated my lipids multiple times and always about the same high LDL (130-190), high HDL (75-103) and low TG (50-70). When I learned about NMR Lipoprofile (LDL-P)I had one performed with results below
NMR lipoprofile results 12/3/2012
LDL-P: 1502 nmol/L
LDL-C: 192 mg/dl
HDL-C: 75 mg/dl
Triglyceride: 52 mg/dl
Total Cholesterol: 277 mg/dl
HDL-P: 36.4 micromol/L
Small LDL-P: 121 nmol/L
LDL Size: 21.6 nm
LP-IR Score: 3
I think I am doing most of the right things with watching my sleep and stress, exercising taking vitamin D and fish oil. I don’t smoke, my BP is 110’s/60’s and my body fat is less than 20%. My hs-CRP’s are consistently < 0.1. Since the LDL-P test, I am restructuring my diet to try to decrease the extra saturated fat. Because of my previous side effects I am a little leery about starting statins again without really thinking about it.
From my limited knowledge it is obvious that my particle number is too high but I can't find any data about patients with similar overall lipid profile. Niacin might be an option but it also has issues and is not often considered a first line agent. Any comments would be greatly appreciated.
Thank you for the post Joe. As carbohydrate restriction and Paleo is becoming so common these days, it is important to understand what happens to our blood lipids with these lifestyles. Although there are a number of short term studies looking at risk factors such as blood pressure, lipids and glucose metabolism, we still don´t know the long-term health effects. There seems to be a general pattern in the lipid response to low carb high fat (LCHF) diets, but there is a lot of individual variation.
Most often, like in your case, total cholesterol (TC) and LDL-C will go up on LCHF. However, this will probably depend on what types of fat are consumed. Saturated fats would be expected to elevate TC and LDL-C more than mono-or polyunsaturated fats. There is usually lowering of TG and elevation of HDL-C, thus the TG/HDL-C ratio improves. We still don´t really know what this means in terms of risk. Will the elevation of LDL-C increase the risk of cardiovascular disease (CVD)? Will the elevation of HDL-C and lowering of TG lead to less risk of CVD? What will the be the net result? Studies are definitively lacking when it comes to hard clinical endpoints.
Therefore the debate is ongoing. Many of the Paleo and carbohydrate restriction theoretics say that TC and LDL-C are not important. They highlight the positive effect on HDL-C and TG and they refer to studies showing that the number of small-LDL-P decreases which they consider important. However, the conventional cardiologist is still focusing on LDL-C and lately non-HDL cholesterol (TC minus HDL-C) and that is what clinical guidelines still recommend. The evidence supporting the role of LDL-C as a marker for risk is very strong and so is the evidence that lowering LDL-C will lower risk.
I agree with you that your situation is indeed very common. If we only look at your lipids we might say that it´s a pity that you can not stay on statin therapy. However, loooking at your total risk, I definitvely don´t think it´s obvious that you should be put on statin therapy. Furthermore, the side effects appear very clear in your case, indicating that the negative effects of statin drugs on your health will be much larger than the positive effects.
Again, looking at your lipid profile, here are a number of positive things. TG are low, HDL-C and HDL-P are relatively high. TG/HDL ratio es less than 1. Small LDL-P is low and LDL size is relatively high.
So the question remaining is how much you should worry about your TC, LDL-C and LDL-P. You probably would want to see all thes numbers a bit lower. Statin therapy would do it, but it´s out of the picture because it will make your general health worse. Looking at your general/total risk profile, the lipids seem to be your only risk factor, apart from the family history. Your healthy lifestyle, absence of hypertension, diabetes and smoking certainly make your total risk quite low indeed. Familial hypercholesterolemia (FH) appears unlikely in your case. The zero calcium score is certainly a positive thing.
Again, many of the LCHF and Paleo theoretics might tell you not to worry about TC and LDL-C, not least because the other lipid parameters look so good. However, looking at the available science on the importance of LDL-C, most cardiologists would probably recommend cutting down on saturated fats and cholesterol. You might try to select more mono and polyunsaturated fats instead. You can still stick with Paleo and carbohydrate restriction if you want to.
Doc, I wonder if you could comment on my situation. Years ago on a very low calorie (starvation diet) with excessive exercise, driving my bodyfat down to 3%, I had 145 total C, LDL-52 and HDL-C 87, trigs 37, glucose 90, crp 0.29. On heavy, but not excessive exercise program and a normal caloric intake evenly balanced between p, c and f, I had total C 185, LDL-C 107, HDL-C 69, trigs 47 and crp 2.0.
Three years ago I went very high fat (75% – 3000 cals worth? ) 20% protein and less than 5% carb (leafy and cruciferous only) total C, 385, HDL-C 87, Non HDL 298, LDL-C 283, trigs 64, VLDC 15, ApoB 184 (don’t have LDL-P), ApoA-1 198.8, glucose 98, insulin 4, my inflammation markers are all ‘borderline’ crp 2.4. diabetes markers are all ‘optimal’.
I don’t know what these are: a-1is 65.5, a-2 is 53.4, a-3 is 18.3, a-4 is 24.3, Pre B-1 is 12.3
The hard core low carb guys say the whole cholesterol thing is a scam (ie take the insulin resistant patients out of the high LDL population and LDL becomes a non-factor) and that total under 500 is nothing, but some say high LDL and totals are ok, but within limits – ie total under 300. and that up to 20% carbs has helped many a very low carb guy not only feel better but metabolize cholesterol better.
To be sure it was diet, I am finishing a month on a low fat diet and expect the numbers to plumet. I was thinking of going low carb-high fat but with all monounsaturates, then the same thing but with only coconut oil as my sat fat to see what it does.
The problem is what if it is a scam? I went on a high fat diet three years ago. I suffered bronchitis and bad chest colds all winter for years – two years ago I added cod liver oil to my diet with the high fat and went two years without a cold (some say that LDL fights infection? and even cancers?)
Any thoughts?
Thanks, Joe
Just got some testing back, after a long period of weight loss and transition from strength athletics to endurance athletics, all the numbers were nicely in their reference range… except that LDL-P, which was obnoxiously high at ~2000. So we’re going back on the simvastatin; but in reading stuff on “metabolic syndrome” which the doc seemed concerned that I might be trying to develop, I see recommendations for a low carb approach. I figure while I’m still used to micromanaging my diet, if I could get a recommendation for ratios (carb/fat/protein) for a 3200kcal / day diet, it’d be easy enough to tweak, while also matching the carbs against times when there’s room for them in recovery of skeletal muscle glycogen. It’d be cool to drag that number back to something sane while not interfering with recovery rate.
I think I will miss the cookie dough though….
I just got my first LDL-P test = 1755. My triglycerides = 48 and my LDL-C = 114. This does not see match the pattern described in the article in that my triglycerides are low and LDL-C not too high. I take 20 mg simvastatin. Take about 3 grams of fish oil per day. BMI around 24. Don’t seem to be a metabolic syndrome candidate. My diet tends toward high carb and my execise level is on the low end.
Not sure of the best course of action in this situation. Maybe someone could comment on this general situation.
Total Cholesterol 365; LDL-C 214; Triglicerides 404; Apo B 189; LDL-P 3500 (yes 3500) What can I eat??? 5’6″, 130#, non smoker, female A little bit scared!
Nette. I don´t know about your age or your family history. Looking at your lipid numbers there is a possibility that you have what is called familial combined hyperlipidemia. My suggestion is that you seek a specialist, either a cardiologist or a lipidologist. Have you done that?
John Male Age 42
Family History – Father had first HA at 46 and is a Diabetic
Ht – 6’3
Wt – 230 lbs (lost 15 lbs in 2 months)
TC 202
LDL-C 106
LDL-P 1667
HDL 57
TRiG 218
Blood Glou 107
After two months of Meditarian diet and 6x a week exercise I dropped 300 from my LDL-P. My NP still wants me to start statin therapy which scares me. I want to keep trying to lose weight. I’m afraid statins will push into diabetes.
John. Your lipid profile is not that bad really and does by itself not support statin therapy, considering that we are talking primary prevention. I agree with you that you should continue trying to lose weight. I think a Mediterranean type diet including exercise is definitively a good option in your situation. This will hopefully help lowering your TG. Indeed, a low carb version of the Mediterranean diet might be something to look at as well.
I have a problematic set of results on my NMR. At least I cannot figure what they mean.
Story: obese most of my adult life; low carb 2.5 years; in first 18 months lost 25 pounds with work; discovered the T2D 1 year ago; added metformin and lost another 10 pounds; weight and BG stuck both still somewhat high; high FBG. In mild ketosis much of the time, with periodic breaks with added carbs.
What does it mean if both LDL-P and HDL-P are off the charts high, IF I am on a long term low carb regimen with high saturated fat with controlled Pre-T2D (a1c 5.8; can’t seem to get it lower), low insulin (6), and good IR numbers; taking 2000 mg metformin. Also LP(a) is very high (137).
Where do I look for what this means? Not theoretical, as my mother had strokes and early-onset Alzheimer’s in her mid-50s. Is the risk real? Can it be managed without drugs?
If you have any suggestions on what to read or where to research, I’d appreciate it. It almost feels as if this is two problems, not one. Or the risk factors have not been vetted against my scenario.
Thanks so much,
Mary
_______________________
The data:
* unexpected results
A1C 5.8
Insulin 6 uIU/ml
LP(a) 137*
B12 331
D 64
LDL-P 2341*
LDL-C 149
Small LDL-P 724
LDL size 21
HDL-P 49.2
HDL-C 88
IR Numbers:
Large VLDL-P < .7
Small LDL-P 724
Large HDL-P 11.4
VLDL Size – not enough to measure
LDL Size 21
HDL Size 9.4
LP-IR Score 15th percentile (good)
@ mpanttaja. As you probably know the high levels of HDL-C and HDL-P are good things in terms of risk. Considering your weight and diabetes I would suspect you fulfill criteria for the metabolic syndrome. So it is a bit surprising that your LP-IR score is this low. Actually, you can often get confused with all these numbers. Maybe you should look at your lifestyle in general and see what you can do to reduce your risk. The saturated fats will not help you lower LDL-C. I wonder whether switching to a more of a Mediterranean type diet, using more monounsaturated and omega 3 fats, might help you. It is a good diet for type-2 diabetes and for weight loss.
Total Cholesterol: 170
LDL-C: 109
LDL-P: 1686
HDL-C: 43
Triglycerides:125
hight 5’7″
wieght:187
I am worried due to my weight and LDL-P ratings. Should I be and what should I do. My overal Cholesterol has dropped from 238 when I was 28 to this number now that I am 48. I take Lipator 10mg.
Thanks
@ Harold. Considering that you are overweight, weight loss probably reduces your risk. Cutting down on sugar and refined carbohydrates often helps lowering LDL-P
Thank you for your thoughts. I believe the IR is under control because of 2.5 years of very serious low carb and a year of metformin. I control post prandial glucose rigorously by eating very few if any carbs. I don’t smoke, I exercise and lift weights, bike to work, ski. I will look into shifting some of the fats to olive oil and avocado and such (from dairy cream and butter), but I don’t think I can increase my carb load as described in that experiment (Mediterranean diet) without raising my a1c. I’m a bit stuck between a rock and a hard place. Obviously, there are some things we do not understand yet. Thanks again for considering.
Thank you for you very enlightening blog. A high LDL-P number often is cited by Drs. Dayspring and Attia as a deciding discordant/concordant indicator of CVD risk. For those in adhering to Low Carb/Paleo, many are confounded when LDL-C has gone up instead of staying low. And worst yet, a high LDL-P number seems to affirm the CVD risk, in concordance w/ the LDL-C level.
A physician who treats those w/ metabolic disorders encountered such a conundrum himself: https://azsunfm.blogspot.com/2012/09/font-definitions-font-face-font-family.html
In Dr. Patel’s premise, a high LDL-P number, in the absence of other risky indicators (TG/HDL ratio <2, fasting blood sugar, low CRP, obesity, hypertension) for metabolic syndromes, by itself, maybe of little value, since other indicators are in the safe zone. A body with low inflammation, there should be no arterial damage from glycation. Therefore, the LDL-P has no injury to deposit its load of cholesterol for repair, thus no plaque.
You take? Thanks.
Hi Peter. Sorry for my late response. I read Dr. Patels article. Very interesting. I think you are right. We often tend to treat laboratory values. We have to see the whole picture. If there are no other risk factors, healthy lifestyle etc, a laboratory value such as LDL-C or LDL-P may be of limited value. We know that inflammation plays a role in atherosclerosis, and we know that lipids do as well. Possibly, turning down inflammation may make high LDL-C or LDL-P harmless. We still don´t know. There are ongoing clinical trials on the effects of anti-inflammatory drugs in patients with heart disease. They might actually provide some answers to the role of inflammation in cardiovascular disease.
“Possibly, turning down inflammation may make high LDL-C or LDL-P harmless.”
Evidence of this?
There’s plenty of evidence of inflammation dying out when dyslipidemia gets treated. It is a pro-inflammatory state.
Lowering lipids is important and will affect risk. But it´s not a one way street. Affecting other risk factors is important as well, and will help reduce risk of heart disease. The importance of lipids as a risk factor becomes less if you can reduce the role of other risk factors.
Hi. I am a 42 year old female. My lipid profile is Total cholesterol 254, triglycerides is 48, HDL is 57, and LDl us 184. My Dr. wants me to take statins, but I want to lower it naturally by exercising, and eating more fiber from fruits and vegetables, and oatmeal. I really don’t want to take statins. Im 5’6 and weight 160lbs.
Good morning Doc. I’m thrilled to have found your blog, after receiving my NMR and Lp PLA 2 labs. There are a lot of FLAGs on the results, so trying to decide if I should see a cardiologist or regular doctor. Your thoughts??
Heart disease runs in my family, with mother having a heart attack in her mid 60’s. She had a stent implanted and no other occurances. She’s now 90! I am also a carrier of the KIF6 Genotype 719 Trp/Arg heterozygous.
I ‘m now 60 and have a similar build to my mom, 5’6″ at 136 lbs. I’m currently not on any medication. I’ve been taking Bios Slim for 1.5 months and have reduced total cholesteral 41 points and have lost 12 lbs. I’ve also implemented better eating habits by eating healthier; steel cut oatmeal, fish, etc. and trying to eliminate all sugars. Also exercising at least 5 days a week for 30 min.
Besides getting my LDL down & HDL numbers up, I was wondering if there is a way to enlarge those LDL & HDL particles. Here are my numbers:
LDL Size 21.0
LDL-P 1712 (high)
Sm LDL-P 833 (high)
LDL-C 134 (high)
HDL-C 44
HDL-P TTL 28.8 (low)
Trigly 111
Chol TTL 200
HDL Size 8.8 (low)
Lg VLDL-P <0.7
Lg HDL-P 5.5
LP-IR Score 31
LP-PLA 196
@ Kathy. Thank you for your post and for sharing your numbers. I have very limited experience with the clinical utility of The KIF6 Genotyping Assay. However, I understand that some studies have shown that statins may be effective for prevention when the KIF6 polymorphism is present, while this was not confirmed by rosuvastatin in the JUPITER trial.
We still have a lot to learn on dietary interventions to lower LDL-P and increase LDL and HDL particle size. Carbohydrate restriction, Mediterranean diet and Omega -3 fatty acids may all be helpful. Avoiding sugars, eating healthy natural fats and exercising are probably helpful. I believe you are on the right track by eating healthier; steel cut oatmeal, fish, etc. and trying to eliminate all sugars as well as exercising. It´s probably more a question of staying focused and keep it going. Good luck.
Hi Dr Sigurdsson,
Would love you to get your thoughts on my numbers. I’m 37, no family history of heart disease, was a social smoker for about 15 years – smoking when I drank alcohol. I started going to a cardiologist about a year go as I was having some random chest pains, he attributed this to stress after a battery of tests – EKG, Stress test, Echo, Echo stress, CIMT but I did discover I had a leaky aortic heart value, mild to moderate leak. During my visits there I got my blood work done a few times and was shocked to learn my LDL-P was 2119! Since then, 8 months ago, I have dropped 20 lbs, starting running 4 times a week and removed all sugary drinks from my diet. I’m very conscious as to what I put into my body. During my last visit, my Dr mentioned going on a statin, would love to get your thoughts on this.
Below are my recent numbers:
Total Cholestrol 165
Triglycerides 81
HDL-C, Direct 52
HDL-C as % of Total 32
Cholestrol/ HDL-C Ratio 3.2
LDL/HDL-C ratio 1.9
Non-HDL Cholestrol 113
VDVL Cholestrol 16
LDL-C Direct 99
LDL – P 1461
Small LDL – P 733
LDL Particle Size 20.6
HDL – P 32
Large HDL – P 5
LP-a 13
hs-CRP 0.8
Lp-PLA2 157
Apo A1 150
Apo B 89
Apo B/A-1 Ratio 0.59
Hemogloblin AIC – 5.7
Glucose – 97
Blood pressure generally around 115/75
Best regards
Mike
Hi Mike.
You´ve certainly managed to improve your LDL-P by changing your lifestyle. Well done, congratulations. To me your numbers don´t look bad at all. Total cholesterol, triglycerides, HDL-C all quite acceptable. ApoB is fine and so is Lp (a). HsCRP is ok. No diabetes. Considering the absence of other risk factors such as family history, hypertension and smoking, the risk of cardiovascular disease in the near future should be quite low. It´s not for me to decide whether you should have statin treatment, but I would consider it very aggressive considering that your general risk is low and your lipids are not that bad really. I don´t think such as decision would be supported by any scientific trial.
My doc insists I am at high risk for a sudden cardiac death if I don’t go on statins right away. She is focused on the LDL-P number (1934) and says none of the other numbers matter. My gyno ran the basic cholesterol test in December, and all those numbers (total cholesterol, HDL, LDL, triglycerides) improved by the time the referred doc ran the Lipid Cascade test in Jan (doc didn’t see me until last week, but called a statin prescription to my pharmacy 6 wks ago. No one told me). Should I continue very low carbing? Should I take the statin? I’m 52 and post-menopause. My most recent A1C is 5.5; my bp typically remains below 120/80 unless I’m at a doc’s office, where it is usually 145/90. Thank you for any clarity you can provide.
Total cholesterol: 274
HDL: 87
LDL: 163
Triglycerides: 66
LDL-P: 1934
LDL particle size: 21.7
LP(a)C: 41.4
hs-CRP: 2.1
LP-PLA2: 253
Apolipoprotein A-1: 225
Apolipoprotein B: 145
@Sylvia
I would not consider you at high risk for sudden death if you don´t go on statins right away. However, I understand why your doctor worries about your lipid profile and assumes he/she may be able to lower your risk by prescribing statin therapy. Total cholesterol is a bit high, so is LDL-choleseterol. Both ApoB and LDL-P are to high. However, when considering risk and potential benefits of statin therapy you have to look at other risk factors as well, such as family history, smoking and blood pressure. You will also have to keep in mind potential side effects of such therapy.
Your hsCRP is just above 2, so according to the JUPITER trial, statins may lower your risk for future cardiovascular events.
Some specialists have claimed that the efficacy of statin therapy in primary prevention may be less in women than men. Dr.Barbara Roberts has written a wonderful book (The truth about statins) where she discusses the pros and cons of statin therapy and suggests that such treatment may be less influential in women than in men.
I agree with your doctor that there are studies indicating that statin therapy may lower your risk of hart attack and stroke. The important thing however, is that you understand the magnitude of benefit, in relation to the risk of side effects. That is something you should be able to discuss with your doctor.
I´m not sure that very low carbing is the best way to go for you. It might be, if you are overweight or have signs of the metabolic syndrome. If we look at cardiovascular risk in general, a Mediterranean type diet may be helpful.
There are exactly *zero* methodologically-sound, clinical trials showing that statins benefit women of any age for any cardiovascular-related diagnosis. Any physician pushing this class of drugs for women is ignoring the evidence, or lack thereof. Whatever problem you might have, statins won’t cure it. Even to say that no other markers matter, like your TG/HDL ratio (yours is outstanding), is not sound decision-making. At the least, you should ask for a coronary calcium test to get a picture of the degree of blockage (if any) in one of your major blood vessels.
Even with LDL-P being the newest darling marker for predicting heart attack, there’s still some question about what the appropriate optimum numeric range is for those on a ketogenic (i.e., less than 50g net carbs/day) diet. In a conversation with Dr. Tom Dayspring, a prominent U.S. cardiac health educator, Jimmy Moore discussed his sky-high LDL-P, and how it was discordant with other markers of cardiovascular health in his case. Dr. Dayspring admitted that there are no good studies of very-low-carbers, and that a different standard might be appropriate.
Hello Doc. Thank you for all this information and for helping all of us. I’m hoping you might help me navigate my husbands numbers… He is 42, about 5’9 and 160 lbs. His father had a major stroke at age 55 and now lives in an assisted care facility. This has obviously been a difficult thing for his family and so this whole cholesterol issue is quite emotional and scarey for my hiusband. We’ve been ‘paleo’ for about 1 1/2 years now. We started with low carb but have increased them in the last few months. It seems his LDL is increasing rapidlyof late. I’m still trying to get the previous lipid panel but this most recent is as follows:
(Values in mmol/L)
Total LDL 6.05 (my husband says that’s up from 4.8 ish last test which was just a standard lipid panel a couple of months ago and since it might be pertinent in considering familial I believe his LDL was within normal limits pre-paleo)
LDL-R 5.15
LP(a) 0.18
Total HDL 1.91
Total cholesterol 8.48
Trigs-VAP .96
non HDL chol 6.57
remnant lipoproteins 1.03
LDL pattern A (less risk)
ApoB100 1.53
ApoA1 1.92
AppB100/ApoA1ratio 0.8
My limited understanding is that apoB predicts particle # (do you know what this apoB number would translate to in LDL-P?) and that this 1.53 is high. However the ratio,which I’ve also read is similar in predictive value to particle number is in the acceptable range. I think his LP(a),trigs and HDL are all good. From what I remember of his previous bloodwork his bp is good, c-reactive p was good, vit D good, thyroid was fine (but I’ve read it can elude standard testing-should we pursue further?). He doesn’t have tendon (or other) xanthomas that I’m aware of. We eat mostly fruit, veg including starchy, well raised meat inc liver and some heart, eggs(mostly raw yolks in smoothie-about 2 yolks/day), lots of canned salmon, high fat raw dairy (cream in coffee, some sour cream..), fermented foods, some raw nuts (and i bake muffins w almond flour), coconut oil. We drink freshly pressed green juice most mornings (spinach, carrot parsley ginger apple lemon). We don’t eat vegetable oils (only olive), grains (except white rice), legumes and very very little sugar and maybe 2-3 glasses of wine/week) Is latent chronic infection a possibility? I wonder about fungal/parasitic and or gut issues (bad dandruff, aggressive belching-even upon waking in the morning on empty stomach), smelly sneezes at times, possibly a little ringworm occasionally and peeling feet very recently -assuming fungal). My oh my I haven’t painted the prettiest of pictures here so you might be surprised to hear that he’s very attractive actually 🙂 looks quite healthy and is in good physical shape-he’s a natural athlete-plus lots of walking, some yoga and I’m pushing him to add more high intensity exercise. Bahhhh! Sorry for the excessively long message. Just frustrated after putting so much care and effort into making good choices and getting results like this. Any feedback on which direction to turn would be helpful. I’m thinking turn more Mediterranean, fish, less chol/sat fat(?) double checking thyroid, and looking into infections… We don’t want to go the statin route if possible-are we putting my husband at risk not going straight to statins as the doctors are recommending?
Thank you so much for your time.
Hi Tami. Thanks for your post. Although Paleo and low carb diets have many health benefits they are certainly not the best diets to lower total cholesterol and LDL-cholesterol. In a normal weight person with LDL-levels this high, I would rather go for a Mediterranean type diet as you suggest, as it might lower cardiovascular risk. I don´t know whether your husband has any family history of premature coronary artery disease. If he had, you would certainly have to wonder whether he has familial hypercholesterolemia (FH). Maybe he should discuss with his doctor about genetic testing for FH. An Apo B of 1.53 g/L is certainly high as well. Under these circumstances, with the high ApoB and LDL-C, most cardiologists would recommend statin therapy. Lipid guidelines usually recommend statins if LDL-C is above 4.9 mmol/L 190 (mg/dL).
Thank you for your reply. I really appreciate your feedback. There is no family history of coronary artery disease, just the stroke as I mentioned above. We will still rule out FH. The interesting thing about this situation is that for the first year plus of paleo his cholesterol rose only modestly-this past reading increased from an LDL of 4.3 to 6.05. I appreciate that there’s a certain number after which statins are recommended, however this rapid surge begs the question why? Is it possible that there is an explanation or cause that should be at least looked for and addressed before artificially lowering the number? I’d love to understand the cause (could diet ALONE cause this dramatic sudden rise when we’ve been eating this way for almost 2 years? If so, then shouldn’t diet alone be able to lower it?).
I understand your concern Tami. You´re wondering why there has been such a change in a short time. Maybe he could try a Mediterranean type diet for a while, and try to avoid animal fats and dairy fats in particular, as well as refined sugars and processed meats, which I´m in fact almost sure he already does. Fish oils and omega-3 supplements may be helpful as well. Then he could have his lipid numbers reevaluated in six months. Sometimes hypothyroidism (low thyroid function) causes elevation of LDL-cholesterol, but I assume this has been ruled out already.
I am 43 with a LDL-p 2530 Total cholesterol was 209 LDL-c 128 HDL-c 52 Triglycerides 199 Non HDL-c 157..
HDL2 7 HDL-P 40.5 elevated hs=CRP 6.23 Fribrinogen 475
Anyway, wondering what diet I could do to lower LDL-p..? I have Hoshimotos, could that make my LDL-p so high.
I am a women 5 10″ 172lbs.
Thanks,
Lisa
@Lisa. You appear to have a typical discordance with an LDL-C that´s not to bad, but and LDL-P that´s quite high. Your triglycerides are high as well. However, to your benefit HDL-C is high as well. There is no particular diet that lowers LDL-P. A Mediterranean type diet may be helpful. Omega-3 may help as well. Reducing carbs may help. The Hashimotos might possibly explain the elevated hcCRP. Hypothyroidism may affect cholesterol levels, but I´m not aware of how, or if Hashimoto´s may affect LDL-P.
I am 60 years old. I consider myself to be in great shape. Most people think I am 50. I don’t smoke, I exercise a lot, I eat what I think is healthy. My numbers are:
Total cholesterol 218
LDL 155
HDL-C 68
Triglycerides 51
Apo B 110
LDL-P 1712
Apolipoprotein E 3/4
MTHFR677 T/T
Omega 3 Total 9.9%
T4 6.9
T3 uptake 37.2
Free Thyroxine Index 2.6
TSH 1.636
Liver and Kidney numbers are good
CRP was 9.8 – must have had infection took antibiotic and it is now 1.6
Lp-PLA 226
Lots of other numbers – not sure what you would want. My doctor wants me to take a baby aspirin. My last doctor said to quit the baby aspirin. That doctor did the Berkley test which showed LPA-AspirinChexk Ile/Ile – not sure if that is why he said stop. What do you think? What else can I do to avoid problems? Thank you so much. Just found this site and it is so informative.
@Judy. I hope you understand that it is very difficult and irresponsible of me give individual recommendations. Therefore I can only answer you in very general terms. If you don´t smoke, don´t have high blood pressure, diabetes, obesity or family history of premature coronary artery disease, your general risk is probably rather low despite the lipid numbers. Of course we would like to see lower numbers for LDL-C, LDL-P and ApoB. Your lifestyle appears to be healthy. Avoiding refined sugars and processed meat will probably help. A Mediterranean type diet may lower cardiovascular risk and may also lower your LDL-P. Lots of fish, vegetable, fruit, fiber and seeds is not a bad idea. Fish oil and/or omega-3 might be a good idea as well.
Thank you so much for responding. I appreciate your suggestions and will work on them. God bless.
Hi Doc! Thank you for this information. I have recently been put on statin and niacin therapy and would like to ask your opinion. I am a 34 yr old female, 5′ 6, 142 lbs. I am heterogenous for prothrombin mutation and MTHFR. I mention this because I recently had a stroke in the ear and suffered SSHL. Here are my numbers:
Total – 174. 3 months prior=174
LDL-C. 108. 97
HDL-C 63. 59
Triglycerides 90. 75
NonHDL-C 111. 115
ApoB 93. 96
LDL-P 1548. 1116
SdLDL-C31. 24
%sdLDL-C 29. 24
Apo A-1 133. 132
HDL2-C 15. 19
Apo B:apo A-1 ratio .70. .73
Lp-PLA2 234. 239
HsCRP 1.3. 20.4
After my test 3 months prior I was put on niacin and baby aspirin once per day. Now my doctor has added pravastatin. I eat an anti inflammatory diet, mostly gluten and dairy free. I’m not a beef eater and never have been. I have a glass of red wine every evening while cooking dinner. I do EVERYTHING right with eating exercising etc. what do you think about this?
Thank you! I never expected to have to deal with this stuff so young….
After reading my post I want to make sure it makes sense. The first numbers after the type of protein, etc are the most recent results taken in February. The second number is from the test taken in December 2012 after the stroke. I’m wondering why some of my numbers went up after being put on Niacin and baby aspirin??
@MomOfTwo. Sorry to hear about your stroke. I guess the main reason you are being treated with statins is the stroke, rather than the lipid numbers per se. In my practice we more or less give statins to all persons who suffer ischemic stroke. However, niacin is much less used in Europe than in the US. If your lifestyle is healthy as you suggest, including exercise and healthy food choices, I guess there is probably not much more you can do. According to the studies on the Mediterranean diet, a glass of red wine won´t hurt. I assume you are taking aspirin or some other blood thinner as well.
Over the past 2 years I suffered 2 PE’s that I think chronic lyme contributed to.
CHD runs in the family
Two weeks ago I ran these tests
Tot Chol 289
LDL 199
HDL65
Trig 143
ApoB 150
LDL-P2410
sdLDL-C 57
Apo A1 154
HDL-P 45
HDL2-C 14
CRP .4
Lipo (a) 31
5 weeks before total cholesterol was 251 and Lipo (a) was 8. the only difference was upping coconut oil and taking a B12/Folic/ B6 supplement.
I am on coumadin due to the PEs and am considering adding 500mg niacin and maybe 500mg Omega 3. I don’t eat junk but am not sure which way to go with my diet, if I should add the supplements (will they thin the blood too much while on coumadin) and how concerned I should be with these lab values? And is it common for Lipo (a) to go from 8 to 31 in 5 weeks? Thanks in advance
Micheal. It is always difficult for me and probably irresponsible to give advice in individual cases so I will try to respond in general terms. I often recommend Omega-3 in similar situations. Lipo(a) is usually stable and not very much affected by diet.Reducing intake of saturated fats may be helpful to get your LDL-C down a bit more. I don´t know about your body weight though or whether you have insulin resistance. Avoiding refined sugars and limiting simple carbs may help lowering LDL-P. CRP is not elevated which is good.
I am a 58 year old with a BMI of 29 and a family history of chd. I have cleaned up
my diet and take fish oil, aspirin, metoprolol and atorvastatin (40mg).
Can you give me any advice on reducing my risk?
My blood work recently showed me in the high risk category as shown below.
LDL-P 1213
LDL-C 64
HDL-C 49
TG 54
HDL-P 27.9
SMALL LDL-P 852
LDL SIZE 20.2
Thank you for any advice.
John. I think your blood work is acceptable. LDL-C is low, probably due to the statin therapy. You are a bit overweight. Reducing refined sugars and simple carbs may help you lose weight and lower LDL-P further, particle size might also be positively affected. Don´t forget to exercise.
I’m a 62 yr old male, 5’9″, 138 lbs . Body fat % around 20%. Have had RA for 15 years (controlled now with Enbrel – latest CRP was .03, HS-crp is also low, sed rates between 1-4), diabetes for about the same time. Control Diabetes through diet/exercise. Had let my diet slip and hba1c had crept up to 7.4. Went on Paleo diet and have brought that down to 5.3. TC is 194, LDL-C is 120,TG are 69,HDL 60. Take 5000 IU of Vit D to keep levels around 50. Also take highly concentrated fish oil (2tsps of Barleans Signature Fish Oil)- roughly 2-4G/day.
My family doctor wants me to go on low-dose statin, primarily due to my diabetes and RA. I’m not really wanting to go in that direction. I requested particle size testing, but apparently the lab manager screwed up the test and once they figure that out, I’ll get retested.
From what I’ve outlined above, do you think I’m a candidate for statins? (both parents lived into their 90’s – had a grandfather on my mother’s side die of heart attack in his mid 60’s)
Thanks so much! All of the comments and your responses have been fascinating and quite illuminating. I appreciate the effort you put into this!
Mark
Mark. The statin issue is always a bit difficult in primary prevention. It would be irresponsible of me to advise you on whether to take a statin drug or not. Your LDL-C is not that bad really, although some doctors might recommend statins because of your diabetes. However, you seem to be controlling your diabetes rather well with diet. Particle testing might help or even measuring hsCRP, though the latter might be elevated due to your RA.
hs-crp was .3, which is quite low, so good there. Am awaiting particle testing results. Recent (4 weeks ago) homocysteine level was 11.4 (4.0-15.4). Any thoughts on that or how to lower it? I’ve read that methotrexate can increase that and I am reducing that (down to 7.5mg/week from 22.5mg/wk), since Enbrel seems to be controlling the RA without the need for methotrexate. I read that folate, B12, and B6 would help to bring homocysteine levels down, but I’m not sure how much I should be taking. Generally, I have been taking 1200mcg of folic acid per day, but I have ordered a better form (5-Methyl-tetrahydrofolate) and will start taking it. I had read that one should shoot for a reading of 6 or below. Not sure if I can get to that point or not.
Both my family doc and my endocrinologist want me to take a low dose statin, but I think that is primarily because that is what they are taught (if you have RA and diabetes,then you at risk and thus are a fool not to take this). I’m just not sure and when I read the possible side effects, I’m even less sure. So I really don’t know who to believe – the docs who firmly believe statins don’t have a role in people with no prior heart disease, or the docs I currently see who might just be afraid to walk out on that plank.
Does the fact that I have diabetes and RA outweigh the fact that I’ve never had heart disease, have BP of 100/60, eat healthy, exercise, etc? Perhaps the particle test will shed some light, although I’ve read that on Paleo diets, # of particles can sometimes be high. I also eat quite a bit of coconut products – I wonder if that would contribute to a higher LDL?
Thanks for helping me to try and figure this out!
Mark
I’m in the center of the U.S. in Missouri and found this site while searching for info on how to determine my cardiac risk. I am due for a blood draw on Friday and have talked to my doctor about getting an LDL-P test (in addition to the normal cholesterol level checks he does) based on some research I have done. He (a general practitioner) knew nothing of the test but with my explanation he agreed that it might be a good idea. I am a 49 year old female following a whole foods/clean eating program which has greatly improved my health and allowed me to lose 85 pounds, drop my triglycerides by over 100 points, and greatly stabilize my blood pressure (which I take prescription meds for). The doc is working with me on reducing the BP meds and monitoring my BP readings. My last blood work showed everything in normal range, but my total cholesterol was hovering at 200 which made my doctor a bit nervous & the level was actually elevated a little from prior checks. I’ve been eating clean with low carbs, almost no sugar, healthy fats (no hydrogenated oils), no artificial sweeteners, and no unfermented soy for almost 2 years now. Do you see any other test that I should ask for, or do you think that if the LDL-P number is low and the rest come back in normal range that I can feel comfortable that as long as I continue to eat this way and exercise that my risk is low? I do have family history of heart disease. Thanks, Janet
I guess I should add…. I started at 250 lbs. almost 2 years ago and am now about 165 lbs. I’m 5’5″ tall. I walk 2 miles & work with light weights about 5x a week. Janet
So, I went ahead and had my doc get the LipoProfile test. He’s not a cardiologist and was unfamiliar with the test that I suggested. He’s happy, but I’d really like an understanding of the values, since my Cholesterol total was borderline according to traditional testing @ 190. Here are my numbers from the LipoProfile. Can you give an opinion/interpretation for me as to what these numbers really mean?
Also, why do these numbers vary from the traditional Lipid Panel testing that he also did (Cholesterol 190; Triglyceride 59; HDL 58; LDL Calculated 120)?? Thanks.
LDL-P: 1335
LDL-C: 132
HDL-C: 74
Triglycerides: 45
Cholesterol, Total: 215
HDL-P (Total): 36.2
Small LDL-P: 386
LDL Size: 21.4
LP-IR Score: 13
59 year old male
I had a my carotid artery cleaned out recently. They also did a nuclear stress test which was fine. I am on 20g of Crestor .mThinking about adding a bile /colesevelam also to lower LDL-p further. I am 184lbs, 5’11”. LDL-P is over 2000, LDL 185 before Crestor. Crestor effects muscles when exersising and when I added Zetia forget it, could hardly walk. Should I take other LDL-P lowering drugs? Is bile seq. a good idea (removed gall bladder years ago). What about a fibrate? I’ll continue the Crestor even if it makes me feel bad. In addition I had low thyroid, but it is normal now since taking Armour Thyroid. I find it odd that I have very low TG and alot of small LDL=P. l Like your opinion.
TG 29
HDL 48
LDL 84
LDL-P 1700
LDL-P size 20.5
Insulin varies 4 to 6
A1c 5.4
Fasting blood sugar varies 82 to 90
I received test results back and have the following: LDL-P 1829, LDL-C 112, Triglycerides 239, Small LDL-P 1088. I am watching my diet and exercising, but would like to know what vitamins would help. A friend suggested fish oil tablets. Suggestions?
I just got my blood test results and am pretty upset that my LDL-P came up unsually high. I am a 54 male 5′ 10″ and a little underweight at 160. I try to exercise once or twice a week. Am eating most organic foods at home but not so when I eat at restaurants. I avoid all fast foods though. I have been taking krill oil for the past year or so. Was told that it was more effective than fish oil. I am very much against taking any kind of statin.
I am relatively healthy and have parents that lived in their 80’s.
Here are my results:
LDL-P 1618
LDL-C 130
HDL-C 41
TRIGLY 140
TOTAL CHOLESTEROL 199
HDL-P 27.9
SMALL LDL-P 794
LDL SIZE 20.4
LP-IR SCORE 55
Well, I got my NMR back today. I’m 5’9″, 136 lbs, BMI 20, body fat% 20. 62 yr old male. I have diabetes (c-peptide score .54, indicating that pancreas is slowly giving up the ghost), and RA for which I take Enbrel. BP is 100/60. HS-crp is .3 . Last HBA1c was 5.3 (I have brought it down from 7.3). Liver enzymes all good. I have been on a low -carb Paleo diet for last 8 months or so. Only form of sugar I eat is small quantities of berries and some very small quantities of 80% dark chocolate. No grains. Mostly wild fish, veggies, salads, nuts, chicken, grass-fed beef. Do use coconut butter in morning smoothies along with MCT oil, avocados,etc. Usually restrict my nuts to macadamia nuts (low omega 6), on rare occasions almonds or pecans. Take 2-4 grams of Barleans concentrated fish oil daily.
It seems that my total cholesterol has risen as has my calculated LDL-C (was around 120 previously). HDL continues to climb since being on Paleo. First time I’ve had this test run, so not sure how my LDL-P particle number compares to where I was before.
Haven’t talked to my family doc about this yet, but know that she thinks my particle size scores were quite good. In the past , she had been suggesting statins to me due to my LDL scores and my diabetes/RA. Not sure what she will decide now
Your take on my scores?
HDL-P 30.5 u/mol/L
Small LDL-P 96 nmol/L
LDL size – 21 nm
Large VLDL-P <.7
Small LDL-P 96
Large HDL-P 10.4
VLDL size – ** (VLDL concentration too low to allow determination of VLDL size)
LDL size – 21.9
HDL size – 9.5 nm
LP-IR score 5
LDL-P 1463
LDL-C 139
HDL-C 65
TG – 48
Total Cholesterol 214
TG/HDL ratio – .74
Thanks!
Mark
PS – I find my LP-IR score of 5 intriguing since I am a diabetic. I assume it must be this low because of how I'm controlling it by diet?
I´m a 55 year old male.I just had an NMR test done and am a bit puzzled by the results:
LDL-P 1340 HIGH (Ref <1000)
LDL-C 213 (Ref =40)
Triglycerides 57 (Ref <150)
Cholesterol, Total 320 (Ref = 30.5)
Small LDL-P < 90 (Ref 20.5)
Large VLDL-P 2.4 (Ref <= 2.7)
Small LDL-P < 90 (Ref = 4.8)
VLDL Size 39.7 (Ref = 20.8)
HDL Size 9.7 (Ref >= 9.2)
LP-IR Score (Ref <= 45)
Here are the results without the reference ranges:
LDL-P 1340
LDL-C 213
HDL-C 96
Triglycerides 57
Cholesterol, Total 320
HDL-P (Total) 45.0
Small LDL-P < 90
LDL Size 22.2
Large HDL-P 15.9
VLDL Size 39.7
HDL Size 9.7
LP-IR Score 15
The LP-IR Score combines the information from Large VLDL-P, Small LDL-P, Large HDL-P, VLDL Size, LDL Size and HDL Size to give improved assessment of insulin resistance and diabetes risk.
LDL-P is somewhat high and LDL-C and TC are obviously very high, but everything else is good. I'm 5'10, 160 pounds, so not overweight, and my blood pressure is excellent every time it's checked. Not sure what to make of this. Thoughts?
Just got labs back.
Total chol 222
LDL-c 148
Hdl-c 55
Trigly 94
LDL-p 1710
Small LDL-p 341
Hdl-p 27.3
LDL particle size 21.5
Lp-ir score 32
LDL c and LDL-p high. Hdl p low. What exactly do these results mean? How can I get the numbers in range? I’m wm 5’10 175 lbs. family history of high cholesterol. Any natural remedies that might work? Coq-10?
Thanks
Diplo. I´m not sure whether you are a man or a woman or how old you are. These factors play a role when assessing risk. You are right, LDL-C is relatively high and so is LDL-P. I wouldn´t consider these numbers extremely bad though. HDL-C is ok, at least if you are a man. Small LDL-p is ok and so is LDL particle size. I don´t think there are any natural remedies apart from healthy eating that might help you improve your numbers. I suggest you analyze your current eating habits and see where you can improve.
Hey Doc
I have been doing paleo for 1 1/2 years. My BMI is 21 and no other health risk. I was doing crossfit religiously for 10 months then got side tracked with a long vacation and personal stuff. Anyways I got my results from my nmr as follows:
Ldl-p 1473
Ldl-c 177
Tc. 261
Hdl-c 78
TG. 28
Hdlp total 30.8
Small ldl-p. 132
Ldl size 21.5
Large vldlp 0.7
Small ldl p 132
Large hdl p 14.3
Ldl size 21.5
Hdl size 10
Lp-ir. 4
Crp 0.34
The CRNP had initially wanted me on a statin with only the basic results done by her:
Tc 222
Hdl 64
Ldl 147
Tg. 57
Vldl 11
Hdl risk factor 3.5
I didn’t want to start on meds. After speaking with my doc he said I didn’t need to and he didn’t want to order the additional testing. He said I wasn’t high risk. So I ordered it online myself. He doesn’t know about the nmr results. Can you enlighten me some on what you think of them please?
Hi there!
I am a 35 year old Caucasian mother of a 3 yr old, 2 yr old, and 6 mo old… Admittedly I have a poor diet and do not exercise… I am 5’10” tall and weigh 140 pounds…both my parents are on meds for high cholesterol… I am a non-smoker and drink socially on weekends – here goes:
I went to a pcp for a physical….sat there for two hours for what took all of 3 minutes and was scheduled to come back to follow up in two weeks.
Returned in two weeks and told them I couldn’t wait that long again bc had to picks kids up from preschool…was told itd be no problem bc the dr was on schedule & they’d also note the chart with what time I had to leave by….after waiting an hour I had to go & asked for a call with my test results.
A month later (yesterday) I call for said results…was told everything was “fine” and they said I could pick up copies of the results.
Just picked them up…everything is not fine bc several lines of results were highlighted for being flagged for being out of range. Could you tell me if I should find a dr to follow up with on those results or just wait until next years physical? Here are the highlighted ones:
BUN/Creatine Ratio: 22
LDL-P: 1761
LDL-C: 136
Total Cholesterol: 215
Small LDL-P: 890
Any advice?
Thanks!!!!!!
Sheila. There is moderate elevation of lipid numbers such as LDL-C and LDL-P. The most important thing for you is to reconsider your diet and lifestyle in general. BUN/creatinine ratio reflects kidney function. It should measure between 7-20. A small, temporary increase can occur during illness or dehydration; the numbers usually return to normal during recovery, but you should have it rechecked soon
Doc,
I would appreciate your opinion on my lipid profile. I have always been borderline and the docs have wanted me on statins but I have resisted (220 total, 170 LDL). Then my numbers spiked a few months ago. After that, I went on low sat fat diet (no red meat, no animal dairy) for 3 months, and my numbers are only marginally better, but the full profile paints a bleak picture (see below). My wife’s numbers did the same. We are like, what the heck? We might as well eat all the red meat we want. Nurse practitioner wants to put me on the strongest dose of the strongest statin (Crestor). That scares me more than my lipid profile.
Before low sat fat diet:
Total: 268
HDL-C: 45
LDL-C 200
Trigs: 115
After low sat fat diet: (I had to pay for the whole profile, the doc would not do it)
Total: 248
HDL-C: 42
LDL-C 179
Trigs: 136
LDL-P: 2283
Small LDL-P: 1460
LDL size: 20.1
HDL-P: 25
Large HDL-P: .9
HDL size: <8.3
Large VLDL-P: <.7
VLDL size: 41.4
CRP: .9
I am 52 years old. Height 6 feet, weight 170 (my Grandpa's nickname was "skinny"). No history of heart disease in family, but Dad has high numbers (but not as bad as mine). Very active, run/sprint 3-4 times a week, or Greg Brooks challenge 250. Fancy scale puts BMI at 23. Eat fish. lean chicken, veges and salad for dinner. Flax seed-chia-spinach leaf-protein powder-spirulina-blueberry shake for breakfast. I watch my carbs (no ice cream, minimize sugary snacks, no sugary drinks-unless you count beer and wine). Don't know what else I could do. I am starting 1/2 a grapefruit a day, as that actually had the most effect in the past, believe it or not, in reducing my numbers (using a home checker).
Thanks
Randall. You definitively seem to be doing everything right in terms of diet and lifestyle. To a large part our lipids are genetically determined. However, to your benefit, there is no family history of heart disease. I´ve seen a number of families where lipid numbers are abnormal but heart disease seems to strike rarely. It appears that there isn’t much more you can do in terms of lifestyle. So, the question remains on whether to take a statin or not. Remember that most people tolerate statins very well. However, there is 9 percent increased risk of diabetes with these drugs. I’m in favor of shared decision making. Discuss with your doctor the possible benefits and the possible disadvantages of statin therapy. The question is always whether the assumed benefits outweigh the risks.
Thanks for your response. What struck me about your response is that you made no mention of inflammation and my low CRP number. If inflammation is the new (or possibly only) “boogeyman” with CHD, then I find it odd that you would not at least mention it. I guess what I am driving at is this: If inflammation is and stays low, can a person ignore lipid levels and stay off of statins?
Randall. I probably didn’t mention inflammation because CRP was fine.
Hi, Doctor:
I just received my lab report and the numbers are as follows:
LDL-P 1003
LDL-C 88
HDL-C 69
Trigly 79
Choles-Total 173
HDL-P Total 42.8
Small LDL-P 655
LDL Size 20.3
LP-IR Score 44
I have slight high blood pressure and taking Lisinopril 5 mg one a day, Simvastatin 40 mg one a day, Metoprolol Er 50mg one a day, and an aspring 81 mg one a day.
I have an ICD (pacemaker + defibillator) due to an episode of ventricular tachycardia in 2010. This is under control and have not had a problem since.
I like to know what you think of my latest lab report with my condition I have mentioned above. I have never smoke, exercise 5 times a week, and drink a glass of wine with dinner. My weight is 160lbs and I am 5’7″ and 61 years old.
Thank you very much for your assistance as this is very important to me.
Miguel
Miguel. I think your numbers are quite good indeed. The effect of simvastatin is best reflected in your relatively low LDL-C. However, if you have coronary artery disease you might want to see LDL-C lower than 70. In that case atorvastatin 40 mg is more effective than simvastatin 40 mg. You could discuss that with your doctor. If you don´t have coronary artery disease or established atherosclerotic disease, your numbers appear very acceptable. I wouldn´t worry too much about the other numbers.
I did as you said and ask my Cardiologist to switch to atorvastatin 40 mg. My results came back and my LDL-C is 63. This is a great improvement. Thank you very much for your recommendation!!!
That’s great to hear Miguel. Wish you all the best.
– Axel
Thank you for your response. Great news! I will talk to my cardiologist on my December appointment about atorvastatin.
I just had extensive lipid panels done and never had the LDL-P done until these labs, and shocked at the high #2216….last year was a bad one as I ate a LOT of deli meats (salami/turkey processed) and too much cheese….so NOW I’m off all deli and cheese.
I also went off Omega 3’s last year, don’t ask. I’m 75, a mess hip replacement keeps me pretty inactive and I’m probably 20lbs overweight….total chol is 237, last year it was 191…could all this processed crap really mess me up? Never smoked, no drinking now and both parents lived to 90+…how concerned should I be.
What about homocysteine, no one mentions this..this year it was 20, last year or so 13…could this be all the processed junk too…….I’m off all that crap.
I eat very little carbs, no breads, no cookies/pasteries and a little bit of ice cream now and then…..will I make it…..
Joy. I don’think you should have to worry that much. Many studies indicate that there is a positive correlation between blood cholesterol and survival in your age group, meaning that those with higher cholesterol have a better survival than those with low levels. Your family history is also benign considering your parents longevity. Nonetheless, healthy food choices are important for you. I agree with you on the processed food, try to avoid that as well as added or refined sugar. Regular walking is helpful and omega-3 supplement is probably not a a bad idea.
I am a 55 year old female, with a BMI of 23. I exercise regularly and have never smoked. The results of my recent blood work showed no thyroid or blood sugar problems. My triglycerides are 97, HDL is 62 and LDL is 148. Due to my LDL number and an overall cholesterol number of 229, my doctor ordered a carotid artery scan which revealed minimal plaque. He wants to put me on a statin. I am apprehensive about taking one, but do not want to put myself at greater risk. I have begun taking a low dose aspirin, per his recommendation and take omega 3 supplements. Does the presence of plaque mean I have coronary disease and would the statin be beneficial?
Terri. The presence of a plaque in a carotid artery does not say anything about whether coronary artery disease is present or not. To me your general risk profile appears relatively benign, you don’t mention family history though. Your lipid profile is not perfect with LDL-C in the intermediate range, but that does not by itself indicate high risk for cardiovascular events. If you don´t have high blood pressure or diabetes, your calculated risk appears very low. So the demonstration of a carotid artery plaque appears to be the main reason why your doctor wants to put you on statin therapy. I would have a discussion with him on the pros pan cons of such therapy. Does the benefit of such therapy in your case outweigh the risk of side effects?
I am 32 years old 5’2 and my weight is 194. I do smoke but I don’t drink. Can you please tell me what does these mean:
Total Cholesterol LDL&HDL&VLDL is 168
Triglycerides linked to increased risk for CVD is 72
Total LDL Cholesterol LDL & Lp(a)&IDL is 94
Total HDL Cholesterol HDL2&HDL3 is 57
non-HDL Cholesterol LDL&VLDL is 111
LDL-P (LDL particle concentration is 1010
I want to know what does these mean? I have three kids that are 12,10,7 and I do want to be around when they grow up. What can I do?. I do workout but when I do my body will swollen up alot
I am so worn out on MD’s wanting to Statin(izing) the world…. I would NOT touch those drugs.
Latest News from Anderson Cooper on CNN last night…..
They had a segment on the “new” guidelines and how they are being questioned by many. Dr. Gupta was talking to Anderson about this and Anderson who is 44 as I recall said he’s been on statins for many years….Claims no muscle joint pain but went on to say his memory is not what it should be, he’s 44 which is young young…
Gupta went on to say 24Million are taking statins and if the new guidelines happen, that number could go to 70Million….I won’t be in that number…..
But if I were in the stockmarket and loved this drug, I’d sure look into the companies who produce statins…I’d NEVER buy stock based on drugs that do harm….
Keep with the Omega 3’s, read some of Weston A Price information on cholesterol/homocysteine….I’ve been an advocate of the Price Foundation for many years…
Keep your exercise program, don’t smoke/little drinking if needed…I’m 75 and I’d love your BMI. The statin world is crazy.
You are so right. Statins, depending I think on one’s genetic makeup, can utterly trash the body, apparently triggering autoimmune diseases. Muscles visibly rot off: I know, because it happened to me after just 6 months on simvastatin. The statin, I now know, might have reduced my chance of CVD by 2% over the next ten years. NIGHTMARE!
Great website and blog. I think I should recommend that the readers check out L-Arginine products for their blood pressure and atherosclerotic concerns. It should improve blood lipids without negative side-effects.
I got quite a shock when my Doctor told me that my bad cholesterol was high. But I found that changing my diet (and maintaining my exercise habit) was all that I needed to do to address the problem. Within 12 weeks, I had successfully lowered my bad cholesterol. It was a relief to know that I had achieved this healthy outcome naturally.
Dear Doc,
A couple of questions for you as I am trying to grasp a better understanding of risk management with regards to CVD.
1. do you think cvd risk (as measured by current medical guidelines) is different for someone with existing cvd vs. someone with undiscovered cvd?
2. If diet , lifestyle, or pharmaceutical changes are made, can progression of cvd be halted (or reversed)?
I have read countless studies, papers, articles, reviews, blogs etc.. that discuss risk as potential development but never clearly addresses the millions of us with diagnosed cvd.
At the age of 49 I was so diagnosed and had 12 stents placed. An athlete my entire life, (symptoms while running on the track triggered a stress test leading to the procedure) I spent the next 6 years on statins and the typically prescribed low fat “heart healty” diet. I was moved from one statin to the next as side affects of muscle cramps, joint pain, and headaches finally became unbearable. Under the theory that inflammation is a primary cause of athero development, I began a strict Paleo diet / exercise program 1.5 years ago. After transitioning to Paleo I literally have never felt better in my life. I have just recently had an NMR done and although my cardiologist is alarmed and wants a return to statins, my numbers are very confusing. I would imagine you have seen this scenario before and would very much like to hear your take on a combination of very high partical number, very high HDL, and very low trigs.
I am now 57 years old, 6’ tall, 165lbs.
LDL-p 2222
LDL-c 240
HDL-c 73
Triglycerides 38
Total Chol 315
HDL-p 29.2
Small LDL-p 161
LDL size 21.5
Lp Ir score 8
Michael. I don’t really think that the approach to risk management should be different depending on whether the person has existing CVD or undiscovered underlying disease. However, if CVD is present our approach in general is more aggressive than if risk factors are present in someone without confirmed disease. I assume that´s the difference between primary and secondary prevention.
I’m sorry to hear about you being diagnosed with blockages in your coronary arteries at such a young age. There is a lot of evidence indicating that statins reduce the risk of new cardiovascular events in similar circumstances. However, I guess nobody really knows whether this is due to their lowering of LDL-cholesterol or their anti-inflammatory or antit-thrombotic effect. I have a tendency to believe that lipid lowering effects of statins may be a byproduct and that their clinical efficacy relates to other mechanisms (pleiotropic effects). However, side effects of statins are difficult to deal with, like in your case, and sometimes these drugs may cause more harm than good.
The lipid profile you present is often seen with carbohydrate restriction and relatively high fat consumption. There are certainly some positives like the low TG and relatively high HDL-C. Of course the high LDL-C and LDL-P is a concern. The traditional approach would certainly be to recommend that you try to lower your LDL-P and LDL-P, possibly by cutting down on saturated fat. I understand that stains are problematic in your case due to side effects.
Maybe a Mediterranean type diet is something you should think about. It allows some healthy carbs and fat is a relatively large proportion of energy consumption. Olive oil plays a large part. However, red meat is limited. This diet is rich rich in fruits, vegetables, legumes, whole grains, fish, nuts, and low-fat dairy products. It seems to protect against the development and progression of CVD. This is actually supported by a lot of scientific evidence.
Low-fat dairy is not part of the Mediterranean diet (it is part of the N. American “Mediterranean Diet”). The significant dairy components of Md are all high fat: Feta cheese is about 70% fat, Greek yoghurt about 60%+ fat (not, of course, N.American “lo-fat Greek-style yogurt”!!). I live in France, not very far from the Med (about 150km/90miles) and our local sheep (& goat) cheeses (no meal without some) are all 40-60% fat. Our local cream is about 90% fat (of which 60%+ SAFA).
Thanks for the comment Kevin.
I don’t disagree with you and you probably know better than I do about dietary traditions in the Mediterranean countries. I’ve often witnessed discussions on what a Mediterranean type diet is. I guess that you can find all kinds of diets in the Mediterranean countries today. What I was referring to is the definition that is most often used in the epidemiological and interventional studies. For example, here is how the concept is defined in the ATTICA study paper: “A diet rich in fruits, vegetables, legumes, whole grains, fish, nuts, and low-fat dairy products protects against the development and progression of CVD. The traditional Mediterranean diet, whose principal source of fat is olive oil, encompasses these dietary characteristics”. So, in terms of nutritional research the term “Mediterranean Diet” covers a certain definition. It is well outlined on the OLDWAYS website here.
Thanks for your reply,
Since 2006 four different elements of the “lipid panel” have evolved into the “first” position as the best way to determine risk and treatment. First it was simply elevated LDL. Then it became a “ratio” factor. After that it was absolutely “particle size”. And now, “certainly” it is Particle Number. I guess we should be thankful for an evolving scientific understanding of underlying cause, but unfortunately this does not bring clarity. So many questions remain and the deeper one digs the more obvious this lack of understanding becomes. I do appreciate your suggestion on tweeking diet (Mediterranean), but I guess one important question we don’t know the answer to is if an LDL-P of 2,000 in someone who eats no carbs is the same as an LDL-P of 2,000 in someone who does. Again, I very much appreciate your insights and will continue to follow your enlightened website.
I think you’re absolutely spot on Michael. We cannot allow ourselves to only look at numbers from laboratory measurements. That may be helpful when looking at large groups but problematic when looking at one individual. I believe as you do that a high LDL-C or LDL-P may have totally different meaning for two individuals. Lifestyle certainly plays a role. What I find most interesting about the Paleo lifestyle is the avoidance of refined foods. I certainly think the inflammatory aspect plays an important role. So, if you choose a healthy lifestyle with a lot of exercise, and take care of your diet, an LDL-P above 2000 will play a much smaller role than for somebody who ignores the lifestyle issues. Statins can never replace healthy diet choices, exercise and not smoking – but they certainly can make your life problematic and sometimes miserable, although they somehow seem to have a protective effect on atherosclerotic heart disease.
Again, thanks for reminding us that it’s not all about the laboratory numbers. It’s about our lifestyle and how we take care of ourselves. Of course there are genetic aspects as well, but must of those we can’t change.
Hi Doc,
I am 46 years old male with familial history of high lipid profile. My recent tests show:
LDL-P 2053
HDL-P 25.6
LDL particle size 20.9
Large VLDL particle number 7.4
Large HDL particle number 0.9
VLDL size 50
HDL size <8.3
LP-IR 73
My LDL-C was always high (150-170); fasting glucose always 105-112, A1C 5.4-5.9.
I have this stupid belly fat that does not want to go away.
After looking at the numbers, do you have any suggestions? I started taking Niacin 500 mg/day and 500 mg of Artichoke Extract. I don’t want to go on statin drug for as long as I can.
Thank you.
Hi Doc..
I am 36 years old male. I am diabetic and Hypertension patient. after medicine both of under control.. jst now my sugar level-fasting 82 and PP-120. My Lipid profile. Total Cholesterol 140. Trygliceride-75 LDL-83 HDL-42 VLDL-15. Is it need for statin therapy.. I am not smoker.
Labs recently came back pretty bad. I don’t eat fast foods or fatty foods but do love sweets. I get regular exercise non smoker or drinker, 35 years old 6ft 240lbs. Outside of too much sugar I don’t eat too bad and I usually struggle to lose weight. Family history is bad too my dad passed away from a MI at 49 so genetics are against me. A statin has been ordered and seems unavoidable. Any suggestions would be much appreciated. Thanks
Results
LDL particle number 2234 very high is >2000
LDL 158
HDL 53
Tryg 161
Total C 243
HDL-P 39.6
LDL-P 1276 high is > 839
LDL size 20.3
Large VLDL 6.3
VLDL size 52.1
Large HDL 2.1
HDL size 8.5
Insulin resistant score 77 should be <=45
To James Buttler:
I know how you feel. Please look into using Niacin (nicotinic acid form only). I have used it in the last two months. I lost 25 Ibs and all my out-of-range lab values are normal (something that I could never achieve even with using statin drugs). See my previous posting on December 20, 2013. Never give up!
Dear Doctor,
This is divakar and my lipid profile is as follows.
Total Cholesterol-145mg/dl
Triglycerides- 172mg/dl
HDL- 29mg/dl
LDL- 82mg/dl
VLDL- 34mg/dl
Cholesterol/HDL ratio- 5.0:1
please advise me about the result
Total cholesterol and LDL-cholesterol are both low which is considered good. However, triglycerides are high and HDL-cholesterol very low. A high triglyceride/HDL- cholesterol ratio is sometimes associated with insulin resistance and the metabolic syndrome. I don’t know whether you are dealing with abdominal obesity or have other signs of the metabolic syndrome like high blood pressure for example. If so, it might help to cut sugar and refined carbs and try to lose weight.
Dear Doctor,
I have been on a strict low carb / high fat diet for the last two months in order to lose weight. The weight loss has progressed great, as I have lost about 25 lbs. (38 year old 6’1″ male 230lbs to 205 lbs.)
While the weight loss is great, it seems to have majorly impacted my cholesterol numbers.
My numbers in 2011:
Triglyceride – 39
HDL – 71
LDL (calculated) – 119
My numbers this week:
Triglyceride – 77
HDL – 67
LDL (calculated) – 330 (!)
Unfortunately, they didn’t test for ldl-p.
Your advice seems to be to cut sugar/carbs, but I’ve had no sugar and no carbs whatsoever for a couple months now.
What might cause this? (Both of my parents are alive, and neither have high cholesterol)
What actions should I consider?
Is it possible to have LDL-C of 330, but still have reasonable LDL-P? (Or is this LDL-C result so far off the charts that my LDL-P must be elevated?)
James
Without doubt, your weight loss has improved your health.
These lipid response is not uncommon on a low carb/high fat diet. Some people respond with a very high LDL-cholesterol and high total cholesterol. However, we don’t know what this means in terms of risk. Although LDL-cholesterol is generally associated with increased risk of cardiovascular disease, we don’t know what it means in this particular metabolic situation. It is quite possible that your high LDL-cholsesterol is harmless, I really can’t tell.
With this LDL-cholesterol, your LDL particle number is most probably too high as well. It surprises my a bit that your triglycerides have gone up. That’s unusual on this type of diet. However, we all do respond differently to low carb/hig fat. If you want to lower your LDL-cholesterol you will probably have to lower your saturated fat consumption, and then replace them by other type of fats, that is if you want to continue with this type of diet.
Doctor;
I am 50 yrs old male, 170lbs, 5’10”, BP 104/70, HR 65, non-smoker, exercise regulary (biking), ski winter. I have a generally sedentary lifestyle when at home and work. Eat healthy (1 cup coffee w/non-dairy creamer, healthy lunch) I tend to eat larger meals after 5pm (meats, veggies-salad) and snack on nuts and fruit at night. My family has very little if any measurable heart disease and typically on both sides live to 85-100+ (depending on marraige and children 😉 ) My dad smoked for 15-20 years and quit 35 years ago and is now 85 and recently had 2 stents put in and is doing great. Other than that not much in family history that I know.
My recent numbers;
LDL-P 2178
LDL-C 182
HDL-C 60
Tri 63
Total 255
HDL-P 39.2
Small LDL-P 796
LDL size 21.2
Large VLDL-P <0.8
Large HDL-P 4.3
VLDL Size nm
LDL Size 21.2
HDL Size 8.6 nm
I am very reluctant to take statins or any medication for that matter. I cannot help but think that my numbers are due to another cause (IBS?) I appreciate any thoughts.
MH
Hello Dr.
I am 38 years with BMI appx 23, non-smoke, non-alcohol, vegetarian with moderate exercise from 3-5 days week and controlled diet for last 3-4 years but still my lipid numbers are not getting improved. Below are my details based on NMR test
LDL-P 1395
LDL-C 102
HDl-C. 32
Triglyc. 183
Choles Total 171
HDL-P 21.4
Small LDL-p 1063
LDL size. 19.9
LP-IR. 74
While lipid PAnel on same blood work shows different values given below
Cholesterol total 176
Triglyecerides 177
HDL cholesterol 29
LDL cholesterol. 112
Please suggest your opinion
Thank you
I took simvastatin for seven short months, 20 mg. I stopped when my lower legs utterly locked up in bed one night. I now have what appears to be a lifetime neuromuscular disease. STATINS CAN HAVE HORRID ADVERSE EFFECTS. Here are some good predictors of who will get their lives destroyed, as I have:
High HDLs, high LDLs, BUT great ratio (mine was under 3)
Low triglycerides, high HDL’s, great ratio (mine was under .7)
Physically very active.
Older (I was 68 and had just returned from trekking in the Himalayan foothills.)
One aspect of the massive statin drugging of our population is who might benefit. But that’s only half the story.
The other, and massively ignored aspect, is who will have their health destroyed: constant burning pain, muscle fasciculations, shocking atrophy, inability to walk or stand for more than 15-20 minutes. In spite of the fact that one of our nation’s astronauts and flight surgeons was trashed by statins, prescribing doctors deny these adverse effects and refuse to report occurrences.
In my case, when I asked, before taking statins, about LDL-P and Apo B, I was told “the science isn’t there yet”. Two separate doctors said the following exact words, “Some people think statins should be in the water supply. Statins are the reason Americans live longer now.” I got an incredibly hard sell on statins. It doesn’t matter to me at this point that the doctors who were selling were also on the drug themselves. The possible adverse effects are horrendous, and although they didn’t get them, I and thousands of others did. I haven’t read of anyone who’s recovered after a year or two, which is where I now am.
I am 61 my hdl is 36 and ldl is 55 is this ok and can you get your ldl to low? Triglycerides is 110
Dan. Your LDL cholesterol is fine, no reason to believe it’s too low. TG are relatively high and HDL-C a bit too low maybe. TG/HDL-C ratio a bit high. This pattern is sometimes associated with insulin resistance and abdominal obesity.
Hi Doc!
I’m 60 years old and overweight. I work out a lot, about 5-6 days/week, but it’s difficult to lose (40 lbs) because I have degenerative disc disease. I eat a very healthy diet that is grain-free, gluten-free, and refined sugar-free. (I have Celiac disease.) I’ve been on Lipitor 20mg for a year because my total cholesterol was 234 on Simvastatin, and I have a strong family history of cardiovascular disease. My only remaining sibling had a “widow maker”, survived, and has a pacemaker in his chest (at 64 years old).
I’ve been reading a lot about “the myth of cholesterol”, and I decided to get a Boston Heart particle test. My results are the following:
Total Cholesterol: 205
Direct LDL-C: 113
HDL-C: 78
Triglycerides: 94
ApoB: 96
LDL-p5: 1288
sdLDL-C1: 31
%sdLDL-C: 27
Lp(a): 120
hs-CRP: 6.7
ApoA-1 a-4: 19.2
Fasting glucose: 136 (on prednisone)
HbA1c: 5.3
I understand this is mixed results. The report says the HDL map is “Optimal”, but I realize the hs-CRP and LDL small particle are not good.
This report was ordered by my family physician, but I’m wondering if I need to get a cardiologist to review this? Not clear if Lipitor helps with small particle LDL?
Thanks for any feedback,
CPowersPHD
Hi Catherine.
You seem to have adopted to a healthy diet and healthy lifestyle in general. However, your numbers, LDL-C and hs-CRP in particular may indicate that there is some residual risk. I would probably not worry to much about particle size in your case, apoB and LDL-P is not bad, suggesting that particle number is not the biggest problem. I suggest you continue with what you are doing in terms of lifestyle. Considering your thoughts on eggs I think they’re fine, nutritious and don’t affect blood lipids badly in most cases. An option in your case of course would be to raise the dose of Lipitor to 40 mg daily. You could discuss that with your doctor.
Also, I read that eating eggs helps lower small particle LDL. Is that true? I’m working on figuring out this diet. And, thanks very much!
Dear doctor,
I’m male 23 years old, 5″5 height and 68kg weight, actively work out 3-4 times a week.
My test result as below:
Total Cholesterol: 304
Triglycerides: 68
LDL-C: 206
HDL-C. 84
What do you think of my result? I find it’s really weird considering I’m still young and active but my LDL so high. Do you have any suggestion for me, doc? I want to check my LDL-P and HDL-P but right now the lab doesn’t provide that.
Thank you.
Newton.
Your high LDL cholesterol is probably an inherited trait. If there is family history of high LDL-cholesterol or premature cardiovascular disease it might be important to react. You should discuss it with your family doctor.
Whoa! Watch out for your family doctor: “high” LDLs almost always result in a statin recommendation. Your ratio of triglycerides over HDL is phenomenally good: this statistically correlates with lower LDL-P (get an Apo B test and see). Especially if you work out hard, your LDLs are likely “large fluffy good” LDLs. If your doc talks about inflammation, ask if there’s a test to determine if you have inflammation (yes, there is). I asked all these questions, and my ignorant cardiologist told me that “the science isn’t there yet”, and hard-sold me on a low-dose of simvastatin. I took it for six months, collapsed, and now have a debilitating neuromuscular disease, apparently for life.
Except for the fact that I’m much older, our data is very similar. When my LDLs got reduced, there were horrifying results. Want photos? reginaofthesun@yahoo.com.
PS In an experiment with older men, weight bearing exercise was prescribed. A surprising effect that no one was looking for: their LDLs went up. What would a neutral (not brainwashed by pharmaceutical advertising and promotion) mind conjecture?
David
You should definitely tell us about your experience with statin drugs here.
Thanks for commenting by the way.
Thank you, Doctor. I have trouble posting where I’d like to–probably my not having figured out the site. When I try to “Reply”, it doesn’t post to the place I expect it to. Oldest comments come up first, and I must scroll through all of them to the newest. Sorry to bother you with this….
If you have personal interest in statin damage, I’d be happy to send photographs. Pretty horrific, and I’m anything but alone in this. David
Doc,
Thanks so much! I’ll speak with my doc and also lower cholesterol foods. Getting f/u testing in 3 months. Thanks for your time and excellent articles!
Dear doc,
No one in my family have high cholesterol except me, that’s why I’m so afraid. I wanted to test apo-A apo-B, and LDL-P, but I’m not sure if this test available in my country, may I know the name of the test method in case they don’t understand. Thank you for your advice.
Newton
The NMR Lipoprofile test which is used to assess LDL-P among other thins is available in the USA. It may be hard to get this test in other countries. Apo-A and Apo-B however should be available in many countries around the world.
In fact, it’s very positive if there is is no history of heart attacks or other cardiovascular disorders at young age in your family. That may indicate that your elevated LDL cholesterol is not harmful. It may also indicate that you should be able to lower it yourself by dietary measures and lifestyle.
The world is in a Panic on cholesterol….read info on the Cholesterol Myth and read up on homocysteine levels and heart disease….. Weston Price Foundation is one GOOD group of health advocates…check their info.
Dear Doctor,
I’ve been having blood tests done for two years trying to get a hold of my numbers. It seems that one number I have yet to change is my LDL-P. It has increased each time I’ve gotten blood work (1791, 1930, 2210, and 2439).
The last two being 3 months between tests. I managed to decrease every other number on my blood panel during the last 2 months as seen below. During the 3 months I went on a low carb diet and dropped 20 lbs. My height is 5’9 went from 195 lbs. to 175 lbs. (32 years old). I would say I am practically in the best shape of my life and exercise around 10 times a week which includes weight training and various cardio.
Total Cholesterol: 251 to 228
LDL-C: 159 to 143
HDL: 55
TG: 227 to 158
HDL-P: 32 to 40
A1C: 7.1 to 6
I am aware and have been told I do have insulin resistance.
I do have cause for concern as my LDL-P continues to rise no matter what lifestyle changes I make. I really don’t want to get on a Statins but fear from not being around for the long haul. As far as I am aware of no family history of heart disease. Just curious to know your thoughts.
@Reggie
It’s quite obvious to me that you’ve improved your health a lot by losing weight on the current diet. Many of your lipid numbers have improved as well and so has HbA1C suggesting less insulin resistance.
I understand it’s disappointing that LDL-P hasn’t dropped. However, it’s important to look at the whole picture and not just one number. Maybe if you give it more time, triglyceride might drop further and eventually LDL-P might follow.
If you eat much saturated fat, you might get LDL-P to go down by choosing other types of fat instead, olive oil instead of butter etc.
Hi Doc! I was so glad to find your site. Really hoping you can give me your opinion. I saw a new doc who scared the living daylights out of me. “Your numbers are really, really bad. It’s scary. If you don’t get on a statin right away, you could have a heart attack anytime! You have no choice” Yet, everything I read about statins seems so scary… and from what I’m finding out, they don’t even decrease LDL-p, which is the number she was focused on, so what’s the point?
I am 43, 5’8″, about 40 lbs overweight, BP 110/70, EKG was great, glucose 93, do not smoke, no meds, moderate exercise 4 times a week, enjoy beer periodically. I believe my maternal grandfather died from heart disease at about 80 years old… other than that, no heart disease in the family and grandparents on both sides live into late 80s/early 90s. I eat healthy, natural food but have problem with amounts.
I am taking the doc’s advice and stictly following the diet she gave me. It’s low-carb, focuses heavily on fruits/veggies and lean meats, relatively low-fat, and instructs me to eat 5 small meals a day. I also thought I would start taking baby aspirin as instructed. That can’t hurt, right? Also, I will get at least 30 mins of exercise every day.
Am I doing myself a disservice if I take 6 months to try to lose 40 lbs before I start the statin? I am quite determined, but not sure if diet can cause the LDL-p to go down. And I don’t want to drop dead tomorrow! I know your opinion is just that and that it’s hard to give advice over the internet.
Thanks for helping so many people. There is so much conflicting information out there and really hard to know what to do.
LDL-P 2185
LDL-C 156
HDL-C 45
Tri 126
Total 226
HDL-P 29.9
Small LDL-P 1439
LDL size 20.1
Large VLDL-P 2.2
Large HDL-P <1.3
VLDL Size 42.9
LDL Size 20.1
HDL Size 8.3
LP IR Score 62
Where did you get all those tests done, and who ordered them? You’re lucky to have all that information as a starting point. Thank you, David
Hi David Venables… not sure if you’re asking me or a previous poster. I started seeing a new General Practitioner and she regularly has all of these tests done for all patients. Ask for a ‘Lipoprotein Particle Profile (LPP) test’ and you should get all the numbers you need. She also did an EKG on my initial visit in order to have a baseline for future yearly EKGs.
What country are you in? I asked for these tests BEFORE taking simvastatin, and was told that “the science isn’t there yet.” This was from a US doctor at the Cardiology Associates of New Haven–right in Yale University’s home town. Pretty sad commentary on US medical care in general.
I’m in the US, howfussiner… NC.
Thank you. My cardiologist in New Haven, when I asked about the tests you have, told me “The science isn’t there yet.” If he’d given me the tests you had, I wouldn’t have taken statins and I’d have the use of my legs today. For some people statins are a true horror drug.
I am a 30 year old female 5’5 130lbs. Do Crossfit 3 times a week as well as take Omega fish oil and flax seed oil supplements. I was told I may possibly need to go on a statin which I am not particularly fond of doing. My question is I’m trying to find the right diet that would possibly help with my numbers, but I’m confused about which would be best since I don’t think insulin resistance is a huge factor . Low Carb, paleo, more whole wheats? Here are my numbers LDL-P 1444, LDL-C 123, HDL-C 72, Triglycerides 57, Total Cholesterol 206, HDL-P Total 33.9, Small LDL-P 132, and LDL Size 21.5, My LP-IR Score was 8. Any advice would be greatly appreciated! 🙂
@ Dana.
These numbers don’t indicate insulin resistance. You’re not overweight either. In my opinion there’s no reason for you to restrict carbs although I think you should avoid refined sugars. Don´t be afraid of fats either but saturated fats are more likely to raise your LDL-cholesterol than mono- or polyunsaturated fats. I would look at a Mediterranean type diet in your case. Eat lots of fruit and vegetables, use olive oil (it´s rich in calories which you may need), eat fish, white meat and I don’t think you need to avoid whole grains.
Dear Doc,
I posted my numbers here short while ago, and you gave some good advice re: talking to my doctor about increasing my Lipitor. However, I just got the bill for the Boston particle test, and it is $2600! I had no idea! I have an excellent insurance policy, but the policy does not cover it, and I didn’t know the expense of the test when my doctor ordered it. Do you know if there is a less expensive way to get a follow up in 3 to 6 months? I live in the United States. And thank you.
@ Catherine
I think LipoScience does most of the testing in the U.S. It doesn’t really matter where the blood is drawn. I believe you should be able to get particle testing for much less money. Of course the cost will depend on which analysis are performed.
Thanks! Which are the most important to get redrawn after an extensive analysis a month ago?
I don’t see a NEED for statins except for the medical industry’s pockets….do a lot of research and check out Weston Price Foundation site…..
My integrative MD has been checking my homocysteine levels the last few years, I am 75 thou and Would NEVER take a statin….. My homo levels have elevated and I’m taking supps to bring them down…..including DHA Max Omega 3’s and homocysteine formula and extra folate….
Personally, I choose to cut out all breads in my home, work with greens to make a sandwich type meal, beautiful organic romaine lettuce….
Hi Doc. I sent the following message and have watched for any advice, but didn’t see a reply. I know you can only answer so many but hoping you’ll get to me… 🙂 Since sending my last message three weeks ago, I’ve been doing low carb and not being concerned with fat. I’ve lost 11 pounds! Thanks!
Hi Doc! I was so glad to find your site. Really hoping you can give me your opinion. I saw a new doc who scared the living daylights out of me. “Your numbers are really, really bad. It’s scary. If you don’t get on a statin right away, you could have a heart attack anytime! You have no choice” Yet, everything I read about statins seems so scary… and from what I’m finding out, they don’t even decrease LDL-p, which is the number she was focused on, so what’s the point?
I am 43, 5’8″, about 40 lbs overweight, BP 110/70, EKG was great, glucose 93, do not smoke, no meds, moderate exercise 4 times a week, enjoy beer periodically. I believe my maternal grandfather died from heart disease at about 80 years old… other than that, no heart disease in the family and grandparents on both sides live into late 80s/early 90s. I eat healthy, natural food but have problem with amounts.
I am taking the doc’s advice and stictly following the diet she gave me. It’s low-carb, focuses heavily on fruits/veggies and lean meats, relatively low-fat, and instructs me to eat 5 small meals a day. I also thought I would start taking baby aspirin as instructed. That can’t hurt, right? Also, I will get at least 30 mins of exercise every day.
Am I doing myself a disservice if I take 6 months to try to lose 40 lbs before I start the statin? I am quite determined, but not sure if diet can cause the LDL-p to go down. And I don’t want to drop dead tomorrow! I know your opinion is just that and that it’s hard to give advice over the internet.
Thanks for helping so many people. There is so much conflicting information out there and really hard to know what to do.
LDL-P 2185
LDL-C 156
HDL-C 45
Tri 126
Total 226
HDL-P 29.9
Small LDL-P 1439
LDL size 20.1
Large VLDL-P 2.2
Large HDL-P <1.3
VLDL Size 42.9
LDL Size 20.1
HDL Size 8.3
LP IR Score 62
@ Shannon
Sorry for responding so late. For a woman your age who’s a non smoker and doesn’t have a sibling or a parent with a history of cardiovascular disease, the risk of having a heart attack in the next 7-10 years is very low. Although I don’t believe there’s a reason to be afraid of statins, I don’t believe they should be first option in your case. I think you’re doing the right thing by trying to lose weight. That’ll improve your triglycerides (TG) and the TG/HDL-C ratio. Hopefully your LDL-C will improve as well on the current diet.
So I would continue with what you’re doing and have a lipid new lipid profile in 6 months.
HDL-C 72, Triglycerides 57??? Don’t even dream of taking a statin! Your tri/hdl ratio is fantastic. Mine was too, and I was as active as you are. Now I can’t walk more than 15 minutes tops. I have a statin-triggered neuromuscular disease. Statins are massively over-prescirbed out of GREED! NOTE WELL: I TOOK 20 MG SIMVSTATIN FOR ONLY SIX MONTHS. IRREPARABLE DAMAGE. PERMANENT, PAINFUL ILLNESS.
Thanks for chiming in David. When I saw those numbers I thought “What crazy quack is recommending statins to that person?” Even for those of us with ratios not quite so good, it should be a long, sober, cautious decision to inflict statins on our bodies just because the BIG drug pushers have deemed it “prudent”.
Has anyone here had any success in treatment for a statin-induced neuromuscular disease??????
I don’t know what part of the country you are in, but have you tried to contact Dr. Barbara Roberts who wrote “The Truth about Statins”?
Yes, she’s great. I own her book and have bought a number of copies for friends. BUT the adverse effect issue isn’t in the area of expertise of a cardiologist. Thanks. I’m in US.
Hi Doc, I recently lost 44 lbs so far basically following a Paleo diet (From 2/11/14 to 5/5/14) (47 y/o male) On 4/11/14 I had a blood draw to check cholesterol and asked doc to ck hs-crp (was unaware of particle# testing at time but I remember asking before if he checked particle size and he said he didn’t do that.) At the time of the blood draw, I had lost about 33 lbs. Results were LDL-C 148, HDL-C 35, Total 199, TG 80 and hs-CRP of 10.89. Needless to say the hs-CRP has freaked me out. The TG/HDL-C doesn’t seem bad 2.2 but again the inflammation as noted by the hs-CRP is a cause of concern. He said he’d retest me in couple of months and wanted to put me on a low dose statin (tried them in the past and I remember having some issues) I declined and said I’d try nature means first. I asked about a low dose aspirin, he said OK but I haven’t tried that yet. I am trying walking more, 1-2 glases of red wine per day, dark choc., tumeric. (all new and doing now after blood draw) Also taking fish oil, vit D3, COQ-10 and some other vitamins but those I was taking before the blood draw too.
Question, I’ve read that cholesterol readings while losing weight could be erratic and should be done after weight stabalizes. Could that also effect the CRP level? Would the new things (walking, red wine, choc, tumeric) help lower CRP level? What is the upstream source of the inflammation and how do I eliminate that? I think I will ask for the particle # next time to have a better picture. I would appreciate any input. Thanks,
@ Anthony
Weight loss usually lowers biomarkers of inflammation such as hsCRP. I believe your right regarding the lipids. I would test them again in a more stable situation. Maybe you will end up being recommended statins, but in my opinion there’s no rush. Have a look at this article regarding diet and inflammation.
Oh, forgot to add that prior to blood draw, had been eating whole eggs (6 to 12 per week), bacon and some hard provolone cheese every now and then thinking that by eliminating grains it wouldn’t be an issue. Since the hs-CRP results, I have curtailed the eggs (only whites), no bacon and very little cheese. Not as happy but hopefully my numbers will improve. Thanks in advance for you reply.
I want to help my husband. He recently had a heart attack, age 55. Almost completely blocked “widow maker” artery, and 50% blocked circumflex artery. He has always had high blood pressure, and a family history of high cholesterol. Nobody ever spoke of the breakdown of the cholesterol numbers…just that it was “high.”
I told him to eliminate carbs (I’ve been doing low carb, high fat) but he is starving. So I thought we’d add back in some gluten free, whole grains. He is nervous about fat.
What is an NMR and a heart scan?
What do we do now that we know he has arteriosclerosis?? He is on the standard meds: statin, beta blocker, blood thinner, etc.
This has been devastating.
Thank you.
Hi Wendy. Sorry to hear about your husband. I don’t think an NMR is a key issue here and neither is a calcium score. He’s already had a coronary angiography and coronary artery disease has been confirmed. I definitely think he should be on statins. Regarding diet I don’t believe whole grains should be regarded as problematic and I wouldn’t recommend a strict low carb diet unless he has to lose weight. A Mediterranean type diet is probably a good option.
Wendy, I’m also sorry to hear about your husband’s present health. Regarding diet, humans don’t require carbohydrates at all. Because grains have changed so much throughout the 10,000 years or so that humans have produced food, I don’t eat them. Grains today are human-created products, and in the format we eat most of them, their glycemic index is often quite high. In a “low carb” diet, one gets plenty of calories. For example, today I ate an omelette of salmon, spinach, two eggs–cooked in palm oil. It isn’t “bulky” food, but I won’t get hungry for six hours or so. There is no carbohydrate hunger bounce-back: no toast, no orange juice=long time not hungry. Missing carbohydrates is another thing, and that can be a balance, I suppose. For health reasons (statin-triggered neuromuscular disease), I’ve been on a low-carb (Paleo, I suppose) diet for a couple of years. Before statin damage (be careful with any statin drug!!!), I hiked and exercised about 10 hours a week: a love of the outdoors, not a health obsession. For two years, I’ve been unable to walk. On the low carb diet I didn’t gain (or lose) a pound; my significant blood measurements (triglycerides, HDL) stayed outstanding. I wouldn’t call my diet “strict” at all. I love the food I eat. David
I’m assuming you eat plenty of carbohydrates in the form of vegetables and some fruit?
I do eat vegetables, but from what I’ve read (examples from people living with the Red Inuits on salmon and caribou meat–extremely healthy as long as the animals had enough fat on them) humans only require protein and fat. There is no need at all for carbohydrates. But one’s diet is certainly nicer, and subjectively I feel (but don’t know) healthier with vegetables. I eat fruit as well, often mixed in with kefir or yogurt. To me, glycemic index is the name of the health game, so I don’t usually eat sweet fruit on an empty stomach.
Oversimplistic, but pretty much do the opposite of what the American Heart Association guidelines recommend. Good read from a cardiologist who stays up on her science: https://www.thedailybeast.com/articles/2014/05/22/the-heart-association-s-junk-science-diet.html#
Given the fiber and nutrients, vegetables are important
And, Esselstyn is showing some interesting results for patients with clogged coronary arteries who he places on strictly plant-based diets
Esselstyn diet would certainly be better than eating any factory food in the USA, and probably most of the world at this point. Farm-raised salmon is usually (always?) a nightmare food; wild caught Alaskan salmon is a superfood. A well-sprayed strawberry is poison; a “clean” strawberry, a superfood. Big Food/Big Pharma: nasty, nasty business all around.
I’ve chosen simply to eat what I’m 99% sure is good for me. Actually, I don’t even think about being on a “strict” diet…unless someone is trying to stuff some birthday cake or something in my mouth. (Yes, it’s only once a year–for each person I know: lots of cake.)
I’d chosen to stay off drugs, but to my profound and lifetime regret, I got simvastatin pushed (and I do mean pushed) on me by my PCP and my cardiologist. Almost instantaneous, lifetime, painful, debilitating damage. You can’t imagine–though I could show photographs. And I personally know two other people with a similar statin-triggered disease. And through websites, I know hundreds more.
I’ve yet to hear of one of these cases reported by the prescribing doctor.
David
Yes I’m sorry to hear that! And, I do understand because I am a nurse. There are risks in taking any medication and unfortunately some people get serious side effects. Personally, I have to eat gluten-free and dairy free, and I choose to eat grain-free. I also eat free of refined sugars. Luckily I don’t have a sweet tooth!
I would call them “adverse effects”, not “side effects”. Regarding the massively over-prescribed statin drugs, I’d call them the only effects–unless one has already had a cardiovascular event there is no demonstrated benefit. Adverse effects are vastly under-reported. I was extremely fit for my age, but statins triggered a debilitating neuromuscular disease in just 6 months: unreported. I personally know two other unreported cases–one being a doctor in the group that prescribed statins to me. His colleagues deny the cause in his case as well–though all three of us had the same immediate symptoms from statins (no, not the mild muscle weakness my doctor said would be what to watch out for); and all of us now have permanent disease. All three of us were very active physically.
Because my life has changed so fast and so profoundly, people ask me why I’m not hiking now, why I’m not swimming, not doing tai chi. When I mention statin drugs, the stories flow. 1/4 of Americans over 40 are on statins, and it’s rare that I hear of someone with no “side” effects at all. I shudder to think what will happen to the 7-year-old child whose mother told me he’d just been put on statins for “high” LDL-C. David
I am a very healthy 49 year old who has worked out for many years 6 days a week. I eat very healthy. Lots of vegetables and lean protein and very little fat. I just got my cholesterol levels and they were very high. 153 LDL and 88 HDL. Total cholesterol was 260. I started taking Apple Cider Vinegar because I heard it helps with cholesterol. Any thoughts?
DANGER!!!!!!
Not to worry! The new “expert” guidelines have raised the level of LDL before statin prescription is indicated. Before was ideally under 100; now prescribe for over 190. As a well know cardiologist from Cleveland Clinic said, “They’re making up these numbers out of the air.”
This LDL nonsense is all about money. Look at LDL-P, not LDL-C, which is what you’re being given. Look at triglycerides/HDL (mine was 7/10).
LDL is a nonsense number, putting the maximum number of people on statins as possible. $30 billion dollar drug.
Your numbers are incredibly outstanding! Great ratio! I was 69 when my numbers were pretty much the same, also very athletic, trekking in the Annapurna foothills in Nepal. Six months on simvastatin and I’m pretty much permanently disabled and in constant pain. You are a prime candidate for a nightmare change in your life.
If you dream of taking a statin drug, contact me first! David
Looks like I’m living on borrowed time. I’m a month away from 49 and my brother just died of a heart attack/cardiac arrest at 62. Just went to the doc to check my blood, and the numbers are not good –
Vitamin D, 25-Hydroxy – 22.4 Range: 30.0-100.0 – ng/mL Flag: L
Glucose, Serum – 106 Range: 65-99 – mg/dL Flag: H
Small LDL-P – 1932 Range: 20.5 – nm Flag: L
LP-IR Score – 78 Range: = 30.5 – umol/L Flag: L
LDL-C – NOTES: Range: <100 – mg/dL
Cholesterol, Total – 266 Range: =40 – mg/dL Flag: L
LDL-P – 2672 Range: <1000 – nmol/L Flag: H
Triglycerides – 434 Range: <150 – mg/dL Flag: H
My doc is going to call something in but don't know what just yet. Based on what I have read above, I need to take Vitamin D, exercise, eliminate carbs. Any other advise would be greatly appreciated, thanks!
Tim. I agree with you a-on vitamin D and healthy diet choices. Avoiding sugar and refined carbs is important. It’s also important to look at the whole risk profile. Getting rid of risk factors such as smoking and high blood pressure is a key issue. With such a strong family history and high LDL-P (LDL-C is probably high as well) your doctor will want to discuss statin therapy. Studies have shown that statins reduce the risk of cardiovascular events among those at high risk.
Aside from eliminating unnecessary harmful carbs like refined sugar and wheat and other things that turn to sugar immediately, I would suggest focusing on all the anti-inflammatory foods. Like vegetables, blueberries and turmeric especially. A friend of mine had an angiogram couple of months ago that was particularly bad and he had several stents put in. His triglycerides were high and his doctor declined to do more extensive blood test. I talked to him about an anti-inflammatory diet that I am on, and he decided to go with that. This week he had another angiogram, and his doctor said he didn’t know why his vessels looked better. I’m not sure how two months without sugar, unnecessary carbs and adding anti-inflammatory foods could have such a result, but it appears to have done just that. He also has very little dairy. And all wild caught fish and grass fed beef, When he eats that. I think he is on a low dose of Crestor, and that did not change. The only thing that changed was diet. Don’t give up! There really are things that you can do to decrease the inflammation in your vessels and to improve your life!
Yet researchers at Texas A&M university found that higher LDL levels predicted greater gains in muscle mass in a strength training study involving 60 to 69-year-old males.
Yes, and researchers somewhere else (was it MIT?), while testing weight bearing exercise for older men, found a surprise side effect: their LDLs went up.
It seems reasonable to guess that this was large fluffy LDL, not dense BB-like.
BUT let’s not anyone know this! It will interfere with Big Pharma’s $30 billion dollar a year statin industry.
“With such a strong family history and high LDL-P (LDL-C is probably high as well) your doctor will want to discuss statin therapy. Studies have shown that statins reduce the risk of cardiovascular events among those at high risk.”
It would be great if your doctor wanted to “discuss” startin therapy, but it’s more likely that you doctor will want to jam statins down your throat, no discussion involved.
Dr Sigurdsson, what “Studies have shown that statins reduce the risk of cardiovascular events among those at high risk?” The first question is whether the studies were funded by Big Pharma: that gives them 500% greater probability of producing drugs that sell statins. Secondly, who defined “high risk”. Thirdly, did the studies produce relative risk reduction or absolute? A 30% relative reduction could be going from 3 in a million to 2 in a million: it could be pretty much anything. But what it always is is a sales tool for statin drugs.
Everything I’ve read indicates that statins may reduce risk for those who’ve already had a cardiovascular event. But no on else.
CAUTION!!!!! In this contest, we need to keep in mind that the “side” effects of statins, many or most unreported, can be devastating. If I could attach a couple of photos, I could show you how horrid the PERMANENT adverse effects can be. Six months on simvastatin (in my case unneeded, as my more up-to-date cardiologist said, “You were in outstanding health before this drug. We see this all the time.”)
Bottom line: there may or may not be benefits. For absolutely certain, probably depending on genetic predisposition, there is a possibility of horrific neuromuscular disease. Constant pain, inability to walk, and…. Well, contact reginaofthesun@yahoo.com if you want to know more.
David
David. There is evidence supporting that statins reduce the risk of cardiovascular events in primary prevention. However, I agree that possible benefits can be outweighed by possible harm. Therefore, the decision to treat or not to treat is not always easy. I believe in informed decision making allowing the patient to have his/her say.
Although I think that the adverse effects of statins are more common than the clinical studies indicate, it has to be remembered that most individuals tolerate statin drugs very well. On the other hand, that’s not an excuse for over-treating. I know for certain that there are many individuals out there taking statins who will probably benefit very little, maybe nothing from treatment. However there are also individuals who may benefit from statins who are not receiving treatment.
I’m really sorry to hear about the terrible adverse effects you’ve experienced. Thanks for sharing your experience. We all need to learn.
Doctor, I’d missed your reply, not receiving it in my email. I’m trying to figure the site out and what I’m doing wrong. I’d love to learn what specific evidence you’re referring to. I’ve yet to find positive evidence from research not supported, directly or indirectly, by Big Pharma.
Adverse effects are almost never reported. I know two other people personally who have devastating adverse effects from statins (and hundreds more from internet sites). One of the people I know is a cardiologist himself, and the change to his health and his life is terrible.
You’re aware, I’m sure, of the BMJ article that Rory Collins was adamant to get retracted (unheard of) due to a statistical error. The actual adverse effects were closer to 10% than the original erroneous 20%. But that’s still 10%–much larger than any benefit number I’ve heard of.
Young Rory has received vast dollars from Big Pharma for research, so I’m not an admirer. But in this case, I think he did some good: we’d probably never have heard of that adverse effect study without Rory’s over-reaction bringing it to the world’s attention.
I appreciate your Website and especially your consistently kind and empathic attitude. David
I am taking Atorvastatin after I asked my cardiologist to switch me from Simvastatin. My numbers are great and I have no side effects. I will not consider stopping this treatment. Be careful of the advise you get from non professionals!
Many people in the medical profession seem to disagree concerning the usefulness of statins in primary prevention. A number also disagree regarding tolerating statins “very well”. I believe that it was an MIT study that concluded an inevitable trade-off between vascular health and skeletal muscle health.
Regarding terrible adverse effects, I’m not sure how aware you are that these are not rare–but they are very rarely REPORTED.
As a matter of fact, one of the doctors in the cardiological group that prescribed simvastatin to me also got seemingly permanent, hugely disabling neuromuscular adverse effects. His colleagues do not accept that this was caused by the statin.Looking at Dollars for Doctors on Propublica, one can see that Merck and Pfizer gave very large amounts of money (for research, speaking engagements, etc) to doctors in this practice: I’m not saying the doctors were corrupt, but they were certainly influenced. This is so commonly the case that it’s odd to find an exception. Commissioned pharmaceutical sales reps descend on doctors’ offices like flies–often, ironically, bearing gifts of junk food.
May I ask a very direct question? Have you ever heard before of anyone else who got massive, life-changing, painful neuromuscular adverse effects from a statin? There are a lot of us! Some of us are physicians. Some, like me, got permanently finished off by a statin drug in just six months or so. None of us received an accurate description of what the early signs were that this was happening–and yet the details of the onsets are remarkably alike.
You are infinitely more informed than the cardiologist I went to. And in addition you seem like a very kind person. I could send you a photo or two and a short video of the shocking things that statins did to my legs. Meantime, as prescribing doctors say to me, “Well you are getting old,” my upper body is amazingly strong for my age (ah, alas, my legs used to be much stronger, but no more).
With every single medication, the risk-benefit ratio has to be considered by the patient and the doctor. When a patient takes statins, I believe it’s their responsibility to know what that risk- benefit ratio is for themselves. Clearly, the doctors need to explain it, as well. Being on statins without adverse effects, I understand this issue. As I’ve mentioned before, I’m also a nurse who worked in cardiology for a period of time. It would seem to me that the people who do develop the adverse effects would be upset, however, surely if they’re educated consumers, they knew that possibility going in.
And be at least as careful of advice you get from professionals.
My prescribing PCP, and also the prescribing cardiologist, both said to me, “Some people think statins should be in the water supply.” Believe me, that’s a vast and ignorant dismissal of the potential downsides of statins–no matter the possible upsides.
More to your point: The next group of cardiologists I saw said, “Some doctors are 15 years behind the science. You were in outstanding cardiovascular health.” The a doctor put his hand on my shoulder and said, “David, sh**t happens. I’m really sorry that it happened to you.”
Are we going to hear about your issues every time this subject is discussed by the doctor?
I think it is important that David has his say. I don’t find him to be nasty. I like to hear both sides of the issue. I’ve had the same comments from physicians that David has heard. I can understand, considering what he has gone through, that he would be a bit adamant about getting his point across. What concerns me is the point David made – how many of these side effects go unreported? If it were me, I certainly try every other method (diet,exercise) before I resorted to statins. I understand that might not be enough for everyone and some might decide to take statins. It’s a very hard call. I have RA and take Enbrel – it took me a long before before I relented and got on that bandwagon. The list of side effects is impressive.
I also am concerned that they are passed out (or so it would seem) like candy. 50 years ago – did we have all these heart attacks from eating high fat, unnprocessed foods? I don’t think so.
My point is that while most people would certainly be empathic to David and his unfortunate position, those of us who are reading this regularly already have been told repeatedly about David’s issues. He brings it up regularly as if we don’t already know this. Once you make your point, I don’t think it’s necessary for the entire group to have to hear the same point over and over again. People who take medications need to take some responsibility for the risk they’re taking when they take the medications.
True. However, I do read everything about the drug I’m taking so in that fashion , I do try to take responsibility. That said, I’m not a medical professional, so I tend to defer to the physician and hope that he has evaluated me as a whole person and is not looking at me as simply one symptom. My experience has not been real positive in that regard. Not true of every physician but true of more than I like to see. I do try hard to let them know the big picture – a lot of it comes down to how good a listener are they.
If your Dr does not consider your entire health in these decisions and does not listen to you carefully about your concerns, I would think you would need a different doctor or at the very least, a second opinion. I spend a lot of time reading extensively about diet, medications, and any factors I can find that would impact my decisions. We cannot blindly trust doctors, lawyers, or anybody. In fact, one of the most disappointing things about the field of medicine is that the typical doctor knows next to nothing about nutrition. No physician ever recommended an anti-inflammatory diet for me, but it is exactly that diet that put and end to crippling pain from degenerative disc disease.
Catherine, I questioned the need for statins in my case. In fact, thankfully thankfully, I resisted the prescription for four years. Trips to all over southeast Asia, even trekking in the Himalayan foothills for weeks, eight-hour days up and down–never out of breath (muscles tired though). I was healthy. In fact, I fit the pattern of many people I know who got crushed by statins.
I questioned the need, but it’s very hard to learn about the adverse effects. Remember, my cardiologist said that “Statins are the reason Americans live longer now.” And some people say statins should be in the water supply.”
What you might want to do as a medical professional is find some research article that says statins safe and valuable as primary prevention, with one caveat: the pharmaceutical industry isn’t involved, none of the researchers have ties to the pharmaceutical industry of any kind.
How can I research adverse effects when they’re not reported? And why aren’t they reported? As yet another doctor said to me, “Reporting adverse effects is made so onerous that doctors simply don’t do it.” One of my biggest frustrations is that my own case isn’t reported. Instead I’ve gotten smarmy statements such as “Correlation isn’t causation.” Duh. But if correlations are reported, then no one will ever looking into causality. And this of us utterly trashed by statins will have no hope.
The neuromuscular specialist I wound up having to see said, “Statins can trigger a disease that you wouldn’t have gotten for 30 years.” My shoulder doctor said, “I see statin damage all the time. It gets me angry.” It’s the prescribing doctors who hang on to their own version of reality.
There is huge controversy around the damaging effect of statins–right now. ABC airs a two-part program in Australia, but the second part gets pulled: in spite of all cautions to the contrary, some people might stop their statin drug. An article appears in BMJ cautioning about adverse effects from statins: immediately doctors with ties to the pharmaceutical industry attach the article.
What I’m saying is simple: statins can, for some people, produce horrific adverse effects. They should definitely not be in the water supply.
Six months on statins. Two years off. Too late now: my health is trashed. I think I was as informed as I could have been.
To repeat: before simvastatin was pushed and pushed on me, I was in fantastic health. Great diet, lots of exercise.
More people die in the US of prescribed drugs than from illegal drugs.
Yes, and what I’m saying is that you have stated this numerous times already. We who read this regularly know what happened to you and know about your hiking, etc. We do have access to the possible adverse effects, which have been known for many years. The information that serious adverse effects were possible were most likely available to you if you did the reading. The frequency of those adverse effects is a different story. And for me, continuing to feel victimized and seemingly angry about this does not help your cause much, In my opinion.
I’ve only replied to replies. Ignorance can be bliss, but not every time. I asked questions to my doctor, and he gave incorrect answers. Yes, I fired him and my new doctors are better informed: too late.
I would agree that the general public should be educated in high school about how to evaluate research results for themselves.
Yes, blame the victim.
If you’ve read what I’ve written, then you know that cases like mine are not reported. You read about rhabdomyolysis and high CPK levels. But unless you go to sites like Spacedoc or SOS, you won’t read and don’t know about this.
You need to do more than ask questions of your doctors. You need to read the research results and perhaps other peoples’ testimonies before taking medication. You keep focusing on you asking your doctor, rather than reading information yourself.
Yes, such as things like this: what does 30% mean, do you think?
DEAR READER: Statins are the most widely prescribed cholesterol-lowering drugs. They significantly lower levels of harmful LDL cholesterol in the body. And they’ve been shown to reduce death, heart attack and stroke risk by up to 30 percent in people at high risk.
Although statins were developed with the goal of lowering LDL cholesterol, they turn out to have at least one other major benefit. They quiet the inflammation that is inside plaques of atherosclerosis in arteries of the heart, brain and other organs. That inflammation-fighting effect also protects against heart attacks and strokes. That’s the reason that recent authoritative guidelines recommend that people with, or at risk for, atherosclerosis take statins — regardless of their cholesterol levels.
Most people tolerate statins without a problem, but statins can cause side effects, including muscle and joint aches. I spoke to my colleague Dr. Jorge Plutzky, director of the Vascular Disease Prevention Program at Harvard-affiliated Brigham and Women’s Hospital, about this problem. Here’s what he shared:
Muscle and joint aches typically go away gradually as your body adjusts to a statin. If not, switching to a lower dose, a different statin, or an every-other-day medication schedule should help.
Another option is to take an over-the-counter coenzyme Q10 (CoQ10) supplement along with your statin. CoQ10 replaces an enzyme depleted by statins. Advocates say it relieves and prevents muscle pain. These benefits have not been proven in rigorous studies, but the supplement is unlikely to hurt you. And it may allow you to continue taking your statin.
There’s another, far more serious, muscle-related side effect of statins that you may be concerned about. It’s called rhabdomyolysis, a breakdown of muscle tissue that leads to the release of muscle fiber contents into the bloodstream. The symptoms of rhabdomyolysis are severe, body-wide aching, severe muscle weakness and cola-colored urine. They leave little doubt that something is terribly wrong.
Still, if you develop muscle aches with statin use, tell your doctor. A simple blood test can tell if your muscle is, in fact, breaking down. If not, your doctor will likely encourage you to remain on a statin because of its tremendous lifesaving potential.
If you simply can’t tolerate statins, ask your doctor about non-statin cholesterol-lowering medications. I’ve put a table listing several cholesterol-lowering drugs, along with their benefits and side effects, on my website, AskDoctorK.com.
Fortunately, I’ve never had a patient who developed the rare muscle problem that statins can cause. But I have had patients who developed mild muscle symptoms. By adjusting the dose, or switching to another statin drug, the symptoms have disappeared.
And while I’ve enthusiastically spoken about the benefits that statins can have, please don’t misunderstand. Statins are not for everyone, and they’re not the only way that people with atherosclerosis, or who are at risk for atherosclerosis, can protect themselves. Regular exercise and a heart-healthy diet are equally powerful, and add to the benefits of statins.
Dr. Komaroff is a physician and professor at Harvard Medical School. To send questions, go to AskDoctorK.com, or write: Ask Doctor K, 10 Shattuck St., Second Floor, Boston, MA 02115
Is not a matter of blaming a victim. It’s a matter of consumers and patients taking responsibility in their decision-making with all of the possible known ramifications. There will always be unknown ramifications because research will always be continuing.
No offense, but when you speak of “my cause”, may I ask what your cause might be?
Or ask what you think my cause is?
I worked in an asbestos factory though college. The owners hired their own doctors, falsified and hid information, caused people to get direly sick and to die. My own good luck or genetic predisposition allowed me to escape unharmed. And those who died, didn’t die until years later. It makes a good story, and in fact became a book which was also serialized in The New Yorker Magazine.
Almost all studies about statins have been financed by Big Pharma. Does one need to say more than that?
Believe me, it’s not just statins. Do you believe that 11% of children in the US should be on amphetamine-like ADHD drugs? ADHD drugs are huge business, but statins are the “blockbuster” drug of all time.
“It’s a matter of consumers and patients taking responsibility in their decision-making with all of the possible known ramifications. There will always be unknown ramifications because research will always be continuing.”
Gee, then we don’t need medical professionals at all!
“Known ramifications”: known by whom. Did you, for example, know that J&J made a defective hip implant? An orthopedic surgeon I know called J&J and questioned them about problems with the device. J&J assured him that there were no problems. So the doctor installed the device in a friend of mine’s hip…but only after having the same implant on himself. They will be winning their litigation, I assume, after hours and hours of paperwork…and of course a second hip implant surgery. They might net $300,000 apiece. What a great deal!
“Research will ….” Research paid for by whom?
No, it’s tiresome to pay attention to your repeated rants on the same issues. Those of us who are informed are very familiar with who is funding a large part of the research.
Thanks for the advice doc! I am eliminating sugar and sticking with low glycemic foods and starting to exercise. Having a stress test done tomorrow to see if any problems already exist. Will discuss statins with my doctor, I have taken them before but it has been a while.
I’ve been vegetarian for over 30 years, and probably as a result of eating so many so-called healthy whole grains, have become pre-diabetic. So, I’ve eliminated all carbs and now find that its hard to keep weight on. I’m thin and very fit (5’10”, 146 lbs, 58 y.o.), and have dropped my A1c to a nice 5.3, basically normal. But my LDL-C is stubbornly high (@120s) and soars to 180 whenever I try to add fish and low-fat cheeses. (I’m one of those people you referred to who can’t seem to handle cholesterol). To keep my weight up, my diet is about 30-40% fats from almonds, peanuts, and walnuts, which I eat prolifically, and some olive oil. In your view, are the saturated fats from these as harmful as an equal quantity of saturated fats from traditionally bad sources, such as dairy products? In other words, is 8 grams of saturated plant fats (found in four servings of peanuts) be similar to 8 grams of dairy fats?
The tradeoff with fish is interesting, as I’m aware it lowers particle sizes, but it does also seem to raise LDL about 10%.
@ Russell – You might find this link of interest -https://paleozonenutrition.com/2011/05/10/omega-6-and-3-in-nuts-oils-meat-and-fish-tools-to-get-it-right/ Personally, I eat macadamias due to their lower concentration of Omega 6 oils.
@cityboys — Thanks for this link, which is a really compelling argument to reduce Omega 6s. But where I am truly confused is that recent, real world studies show that higher nut consumption is inversely correlated with lower total and all-cause mortality (including CVD issues). I think something is missing in these theoretical arguments against the Omega 6s in nuts and seeds. Perhaps its the fiber or other phytochemicals in the nuts with cardioprotective benefits. See: https://www.nejm.org/doi/full/10.1056/NEJMoa1307352
LDL-C is the crudest measurement for cardiovascular risk: but it sells statin drugs. LDL-P is much more meaningful. Or look at triglyceride/HDL ratio. Or other tests–available, but not profitable in terms of selling drugs. Triglycerides are more meaningful, but there isn’t a drug to lower them.
One interesting observation regarding LDL-C. A study put older men on weight-bearing exercise. A unanticipated effect: LDL-C went up. That to me provides much food for thought regarding LDL. I don’t think weight-bearing exercise is bad; I think some LDL’s are actually very good.
@cityboys — You may also appreciate this from the Harvard Health newsletter about nuts. Regular nut intake may reduce sudden cardiac death by 47%, and from all cardiac causes by 30%. One of the studies was based on 2.2oz/day (without specifying which nuts), which is very high intake and suggestive that Omega 6s in nuts may be harmless (at least, that’s how I interpret it, though I’d love to hear Axel’s thoughts). The article points to increased arginine, which increases nitric oxide, which supports endothelial health:
https://www.health.harvard.edu/newsweek/Nuts_and_your_health_Cracking_old_myths.htm
Throughout my life, my LDL has always been high, my HDL has been high, my triglycerides low and my total cholesterol high. I do not smoke and I have a family history of CVD and heart disease (my sister had stroke at 45 and mother at 78). I was on statins (Crestor 20) for 5 years and stopped as I wasn’t feeling well on that medication.
At my request, my family physician ordered the detailed LDL tests.
Results are as follows:
LDL-P = 1947
LDL-C = 223
HDL-C = 75
Triglycerides = 133
Total Cholesterol = 325
HDL-P = 37.4
Small LDL-P = 123
LDL size = 22.0
LP-IR score = <25
My doctor thinks because my LDL-P and LDL-C were high, that I have a real problem. She didn't mention anything about the small LDL-P and she did not give me the test results until I left the office.
Please help me decipher this.
Thank you
Jan
@ Jan
Sorry for the late response. It can’t be argued that your LDL-P and LDL-C raise some concern. HDL-C is ok though. Of course many doctors and clinical guidelines would recommend statin therapy in order to reduce your risk of having a cardiovascular event in the future.
You can also reduce your risk by lifestyle modification. Staying away from sugars and simple carbohydrates may lower your triglycerides and raise HDL-C further. If you are overweight, losing weight may help reducing your risk and will improve some of your lipid parameters as well.
I would recommend you limit the intake of saturated fat. For example, use olive oil instead of butter. Omega 3 may help lowering triglycerides. Regular, moderate exercise is helpful.
So, in fact there is quite a lot you can do. Discuss the statin question with your doctor. He might suggest you try a lower dose of Crestor. Just a thought 🙂
Oh, and I do not have high blood pressure. And I’ve lost 10 lbs in last several months from eating healthier and exercising.
What is the reference range for” HDL-P Total”?
Dear Mr. Sigurdsson,
First let me commend you for so willingly giving of your time to respond to everyone’s inquiries and for having a more balanced approach over the drug pushing doctors I often encounter. I am looking for a doctor with a similar approach, but in the mean time I would love to share my story and hear your opinion.
I suspect that I have FH. I am not 100% sure I have it, but there is a good chance because my father does, or at least that is what his doctors have been telling him. I still need to rule out hypothyroidism (which my mom has), but I am fairly sure one of the two is affecting me. Here’s a little history if anyone is interested…
My dad had a triple bypass surgery at 30 and numerous procedures since. His dad died of heart attack in his 50’s, cousin had a triple bypass at 18, his uncle died of heart attack at 32 bending over to tie his shoe, and even his mom had a stroke at 60.
I was vegetarian for 15 years, during which time I ate 90% organic, lots of whole grains, some dairy (not raw) and no eggs, ever. After 3 pregnancies/nursing relationships I felt totally depleted. I started eating eggs, then raw dairy and now grassfed meats/organs/fermented cod oil and lots of vegetables and some fruit (we raise most of our own meat and veggies and fruits).
I had trouble digesting, still low energy (but better then when vegetarian) and generally not feeling as good as I should for being 36, fairly active (have a farm), still was ~ 25 lbs over weight. Last summer I did full Paleo, no grain, no milk, no sugar for 2.5 months coupled with High Intensity Interval exercises 2x week, sprints 1x week, some weights, and walking and of course farm work. I was also still nursing a toddler. I gained several pounds on this protocol and really began to be suspicious. Plus my LDL went up 100 points in 4 years since decreasing carbs and adding meat/eggs.
A paleo/Wapf nutritionist/metabolic typing friend had me do some blood work, then a modified GAPS for three weeks to cleanse my gut (less fat, lots of geletin, bone broth, well cooked veggies, stew, no fruit, no raw food). My LDL went up 23 points in two months to 261. Here are my numbers:
Vegetarian 2010 3/14/14 (Paleoish) 5/22/14
Total Chol. 199 294 312
Triglycerides 74 65 45
HDL 45 43 42
LDL 139 238 261
Total:HDL 4.4 6.8 7.4
LDL-P – – 2541
Small LDL-P – – 564
LP-IR score – – 38
So my Triglycerides went down, so I am thinking it is not infection or insulin resistance.
I am very healthy at 64 years old. I exercise, do Yoga, eat great, have an HDL of 90 but overall my cholesterol is 198. The doctor says it is genetic and I should go on a statin. Do you agree?
@teacherwritermother
Your calculated Non-HDL cholesterol is 108 which is very good.
If you don’t have any other risk factors (smoking, high blood pressure, diabetes, first agree relative with premature coronary artery disease), I would not recommend statin therapy.
Dear Teacherwritermother: Your doctor is nuts. Crazy. Uninformed. Dangerous! Statins are not safe drugs: many of us have gotten permanent severe myopathy from statins. But even if one doesn’t choose to acknowledge that horrid fact, the new “expert” guidelines regarding statin prescription for LDL is a level of 190 or higher. DANGER! (I agree with Dr S that there might be exceptional circumstances, but you don’t mention any, so….)
I’m thankful that I tolerate statins because I need them.
Not trying to pry, but what makes you think that you need them? If it’s LDL-C under 190, the new guidelines don’t recommend statins.
Dr. Sigurdsson,
Many of us spend a lot of time trying to figure out how great our risks are based upon our lipid profiles and particle sizes, but I’m wondering if there is another, faster option. Wouldn’t it make sense to do a non-invasive carotid artery sonogram instead? Low cost, easily done, and from what I’ve read — correct me if I’m wrong — there is a 96% correlation between carotid artery plaques and plaques in and around the heart. So for example, if a carotid sonogram shows zero blockage, many of us would save a lot of time trying to figure out whether our current diet is optimal, or not. Teacherwritermother, and many others here, including me, would also have less anxiety about this issue. 🙂
Thank you for your thoughts.
Russell
@ Russel Long
Thanks for your comment Russel. Assessing carotid intima-media thickness has been used as a surrogate end-point for atherosclerosis in many studies. There is a relationship between this parameter and the severity of atherosclerosis elsewhere. However, although the method is relatively cheap and easily performed, it has not gained widespread use in clinical practice.
Whether carotid intima-media thickness can be used to target therapy or monitor the effect of dietary/lifestyle choices is not known. However, I wouldn’t be surprised if this method would gain more popularity in the near future.
Another commonly used method to assess risk is measuring coronary calcium score by computerized tomography. Although coronary calcium score is a strong predictor of risk, it involves the use of X-rays, exposing the patient to some radiation, which is a disadvantage.
Hi Doc!
Wow…very confused. Just got my VAP results today :total cholesterol: 291
triglycerides: 132
total LDL: 180
total HDL: 82
non HDL: 210
LDL-P 1916
Lp(a) 20
Direct Lp(a) immunoassay: 298.7
Apo al:199, Apo B: 129 ApoB/Apo Al ratio: 0.65
LDL 4+3+2+1 =136, VLDL3 =19, total VLDL = 29, LDL density: A
I am 57 female, overweight, active lifestyle. non smoker. BP: 124/82 (today), Blood glucose: 107. Father had angioplasty @ age 57..no other history. My Doc wants statins…due to Lp (a) of 20..which he said coupled with 291 cholesterol and LDL-P 1916 indicated change of lifestyle was not a choice. I had suggested giving me 3 months to “change the numbers”.My question….Am I crazy to try my idea??
Want to Thank You…really got allot of good info from your site,,,and appreciate your response very much.
Thanks.
Cathy
Except that my triglycerides were 70, your numbers are very close to what mine were before statins. After 4 years of resisting taking a statin, I took one for six months and now have myopathy to the degree that I can’t walk. It is a nightmare, painful and permanent disease. Check out the Stopped Our Statins group on Yahoo, or Spacedoc.com to find out how many others this has happened to.
If you’re physically active (I hiked intensely for about 10 hours a week and did calisthenics, etc), you can try dietary changes before statins. The benefits of statins may or may not be true: for sure many cardiologists think that for older women (I’m 14 years older than you, but am a man), statins bring no benefit.
But for absolute certain, the almost-always unreported adverse effects of statins can be horrific.
Cathy
Of course change of lifestyle is a choice and can have profound effects on lipids. CVD is a very complex disease and there are many markers that can signify an issue yet in others, those same markers that may be high, cause no CVD. So you can see how difficult it is to pinpoint one thing. Our genetics drive so many different variables. They even drive to what extent one may tolerate statins or not. And I also know many on statins with absolutely no side effects and have had profound reductions in numbers like LDL-P.
But it doesn’t mean statins are the only option. I got big reductions through diet and Zetia because I am a hyper responder to fats…but its taken me a year of self experimentation to find out what works through rigorous testing. What works for me, doesn’t mean it will work for you.
Dr. Sigurdsson,
Thanks for your thoughts on this. Yes, I’m aware of the efficacy of coronary calcium scans, and understand the concerns that the radiation risks may be a bit excessive for many of us who don’t have other highly obvious risk factors. My back-of-the-envelope analysis suggests about six times more exposure than a typical single-view chest x-ray, and given that the diagnosticians recommend a baseline and a follow-up scan a year later (and potentially more after that), both the high cost and the potential exposures appear to be non-trivial. This is one reason why I thought that carotid scans may be more efficacious both on cost and radiation exposure measures.
Appreciate your support for this view.
Russell
Howfussiner,
“Statins are not safe drugs: many of us have gotten permanent severe myopathy from statins.”
Muscle pain (prevalence 10%, a small fraction of all the cases severe) vs reduced risk of MI, stroke etc. etc.? I’d say that on population level it’s kinda obvious which way to go, if and when we’re talking about CHD patients and/or high risk population (that is, people who should be prescribed statins in the first place). And if you’re statin intolerant, there are always options:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3138147/
https://www.lipidjournal.com/article/S1933-2874(14)00158-5/fulltext
I suppose it’s “obvious which way to go” unless and until you are one of the unfortunate statistics hobbling around with severe myopathy.
Pretty much any kind of medication has side effects. It’s a matter of weighing the potential benefits vs potential harms.
And of course you read the links about how to deal with the statin intolerant?
I never had cardiovascular problems. I was in the “risk” group because of LDL level. The new “expert” guidelines (AHA, AAC) raised this level recently to 190 before statin prescription recommended. But my present doctors don’t even know this.
The new guidelines put 1/2 of Americans over 40 on statins. Does this make intuitive sense?
I don’t know what diseases statins might prevent. The Jupiter study (who paid for it, do you know?), said statins reduced cardiovascular disease. But it also says (Table 3) that the subjects who took statins had a 50% higher mortality rate than the placebo group.
I write this as one of millions who were given statins because “they were safe” and “were the reason Americans now live longer”. They may benefit the appropriate people (not 1/2 of Americans, I don’t think): but they bring horrid, life-shortening disease to others.
Are you aware of how strongly suppressed any discussion of statin’s adverse effects is? Look at the recent BMJ/Rory Collins … I’d say “scandal”.
I’d like to see a reference for that “50% over 40-year-old Americans”. And for the record, I myself don’t agree with the new US guidelines on a few issues, including the reference level for the start of statin therapy.
As for JUPITER, it really shouldn’t be a surprise that drug trials are funded by drug manufacturers. Why, do you have a better solution? They are independently monitored, however, and the results are open for criticism. For some reason, criticism on the net usually stops here – without inspecting the study itself, even though this is of primary importance (funding, at best, of secondary interest and only if there’s something wrong with the study, reporting etc. itself). Or if it goes further, it’s just plain … Well, incompetent. I’m looking at Table 3 in
https://www.nejm.org/doi/full/10.1056/NEJMoa0807646
now and your claim is simply not true: the treatment group had significantly reduced death rates. Care to explain what on earth were you trying to do here?
As for the “discussion suppressed”, you’re referring to the withdrawal of Abramson et al, well, that was simply because the paper had a serious error in it. But of course Collins cannot be right as CTT gets funding from Big Pharma!
(Notice the lack of any rational attempt of PROPER criticism of the matter and/or the neglect to disclose the fact that statin skeptics tend to have financial interests involved in these matters too).
Thanks, Mie!
I take statins and my numbers are very good and I feel great. You can’t go by everything that is out there. I am seeing a lot of alarmist against statin. But, at the end of the day is your decision, mine is taking statin. If you are going to look at the negative, then stay home and don’t leave the house because getting in a car can be very dangerous!!!
Yes, I also felt incredibly, wonderfully great, until after 5 years I finally gave in to the pressure to take statins. At 69 years old, I was running up mountain switchbacks, training for a trip to Everest Base Camp. Now I can’t walk.
But the point I’ve been trying and trying to make is that my doctors refuse to report this adverse effect. I’m not asking that they say that statins caused what happened to me (though from the thousands of others it’s happened to, I’m almost sure it did). But I admit that I can’t be certain.
I’m just asking that the doctors report that this happened to me. The doctors say with certainty that what happened to me wasn’t caused by simvastatin. That is anti-scientific. They can’t possibly know.
So they should report it, and if there are thousands and thousands of others, we can try to find out what’s going on.
PS Regarding timidity and staying home, I’m not sure that I’m timid, but I am pretty much reduced to staying home. I wish you could have accompanied me a couple of year ago, just a few months before taking statins, on some adventure trips to India, Nepal, Cambodia, etc. I often travelled alone, scramble up temples in Angkor Wat where a newly made Cambodian acquaintance informed me that two foreigners had fallen and died earlier that year. I did not want to get hurt, but I’ve never minded risk. But what happened to me is like getting electrocuted by your telephone or something. Or getting killed in a GM car. (Hope you don’t work for GM.)
I can quickly answer just this part for now: “Why, do you have a better solution? They are independently monitored, however, and the results are open for criticism.”
1. From Harvard School for Public Health: studies sponsored by drug companies are five times more likely to find results beneficial to the drug company. (Can this really surprise you?)
2. The “results” aren’t open at all. The raw data is “proprietary”, so that no one else can actually study or interpret it with independence.
3. Yes, a much better solution would be studies sponsored by NIH or similar.
For free, a number 4: Nixon’s been in the news recently, including how his Surgeon General was fired for saying flat-out that tobacco was harmful to people’s health. He was supposed to go along with the tobacco industry’s contention that this was still open to medical debate. All I’m saying by this is old knowledge: follow the money.
1. I know. There are several explanations, although you’ll probably ignore everything besides the same ol’ “Big Pharma lies” story. For instance, these studies are larger (more statistical power) and deal with the “core population” (those most likely to benefit from the intervention, eg. in the case of statins, those with CVD).
2. If there’s something strange going on, this’ll most likely be evident from the research article itself, in which case further investigation starts. Not to mention e.g. FDA monitoring the case. Or the fact that if the results can’t be replicated, then … Well, the same as above.
3. Care to explain where you’d get them the kind of money required to sponsor the amount of Phase III trials all the drug companies carry out every year? Do you even knkw how much money all that would require?
1. I never mentioned “Big Pharma lies”. I’m trying to stay away from simplistic inflammatory statements.
People who’ve already experienced a cardiovascular event may very well benefit from statins. I don’t know, and I don’t need to know. But I would never suggest that someone who had had a cardiovascular event stop statins.
What I do know is that studies funded by a drug company are five times more likely to find results beneficial to the drug company. Does this really surprise you?
The recent “expert” panel, in setting guidelines for statin use, raised the number on statins form the present 25% to a recommended over 40%. Many on the panel have ties to the pharmaceutical industry. Obviously only a fraction of the 40% have had a cardiovascular event.
Even statin a strong statin advocate responded to this panel by saying, “They’re making these numbers up out of the air.”
2. Actually that “something is going on” is evident from the studies themselves. This is true even though the raw data from the studies is “proprietary”: I can only wonder what the raw data might reveal.
If you like, I can show some ways in which the studies are deceptive. You know what relative numbers vs NNT are, no?
3. Personally, I’d have studies funded by those who don’t benefit or lose financially depending upon the findings of the studies. Research used to be funded my the NIH, which I think is a good idea.
It’s only relatively recently that academic research has been funded by private pharmaceutical corporations–and thus distorted.
Not sure what you mean by “how to deal with the statin-intolerant”.
Why does one want to “deal” with us, and most especially if we’re over 70 years old and healthy?
Gee, perhaps it might have something to do with the articles I linked? You know, the ones dealing with how to treat those intolerant to statins?
Again, treat them for what? Do you think older people with higher than normal cholesterol have a higher mortality rate than those with lower than normal? Nope, it’s the opposite.
So I’m not being facetious: treat them for what?
https://www.nytimes.com/2013/11/13/health/new-guidelines-redefine-use-of-statins.html?pagewanted=all One in four now on.
https://www.nytimes.com/2013/11/14/opinion/dont-give-more-patients-statins.html You may be right: not 50%, maybe just 42.5% Sorry for the (slight) exaggeration.
Disclaimer: I have no association with any pharmaceutical company involved with statin drugs.
Oh dear … Yes, 25% of people over 40 are on statins, that is stated in the first article. In the second article, Abramson (besides repeating the mistake of the paper he co-authored) states that his estimate is that the number of “healthy” (meaning primary prevention) people on statins would increase 70% because of the new guidelines.
Now, this doesn’t mean that 42,5% of those over 40 will be on statins as the 25% on statins now ARE NOT all primary prevention patients.
Oh dear, you’re right. But as with the BMJ scandal, the correction number doesn’t alter the conclusion: the vast majority of those on statins have not experienced a cardiovascular event.
Rough numbers (I’m happy to be fine-tuned): say 1 million or even 2 million US people have had a cardiac vascular event; about 32 million are on statins. (These numbers aren’t wildly off.)
So about 95% of those on statins haven’t had a cardiovascular event. So feel free to tweak the 42% percent number to that extent.
I don’t claim to know about the 5% above. I’m talking about the 95% or so (30 million people) who are prescribed a drug to prevent something they haven’t had. (Yes, I understand that vaccines are used this way too.)
The question is what happens to these 30 million people. I know what happens to some of us, and I know that it can be absolutely horrid. I know of thousands of us sickened like this; and I only know of one who’s had her case reported to the FDA by her prescribing physician.
This doesn’t have to be a win-lose argument, you know. You know my motivation for posting here. It might help if I understood yours a bit better.
This isn’t an inflammatory question: What to statins do, positively and negatively, to the 95% of statin-takers who’ve never had cardiovascular disease.
That’s a given
In my case it is. In the doctor who prescribed statin to me, not so much. On Pro Publica anyone can learn of the hundreds of thousands of dollars his practice received from Merck and Pfizer. I’m not implying that he wrote prescriptions for profit: I’m saying that he was influenced in his opinions. Just as he was influenced by the parade of pharmaceutical salespeople trekking through his offices.
Howfussiner:
“Again, treat them for what? Do you think older people with higher than normal cholesterol have a higher mortality rate than those with lower than normal? Nope, it’s the opposite.”
Treated for the increased risk of CVD.
You’re referring to a well-known case of reverse causality: in cohort studies elderly people with lower total cholesterol have a higher risk of death because low cholesterol is a marker of e.g. poorer nutritional status, cancer, frailty etc. etc. However, if you’ve been treated for increased risk of CVD for years, high LDL doesn’t magically turn good just because you reach a given age.
As for statins, of course the issue of benefits vs harms is somewhat different in the elderly. Statins and the elderly:
https://circ.ahajournals.org/content/115/6/681.full
Even in lower risk primary prevention statins reduce the incidence of MI and stroke among older people:
https://content.onlinejacc.org/article.aspx?articleid=1732396
Here’s actual data in terms understandable to me as a layperson:
Primary prevention (those without pre-existing heart disease)
Statins do reduce the risk of cardiovascular events in people without pre-existing heart disease. However, this effect is more modest than most people assume. Effect of statins given to people with no known heart disease for 5 years (5):
•98% saw no benefit at all
•1.6% (1 in 60) were helped by preventing a heart attack
•0.4% (1 in 268) were helped by preventing a stroke
•1.5% (1 in 67) were harmed by developing diabetes
•10% (1 in 10) were harmed by muscle damage
These statistics present a more sobering view on the efficacy of statins in people without pre-existing heart disease. They suggest that you’d need to treat 60 people for 5 years to prevent a single heart attack, or 268 people for 5 years to prevent a single stroke.
And this refers to men and women. If you analyze women separately there is NO benefit on heart attack, stroke or death.
Barbara
Barbara Roberts, MD
The numbers are from NNT.com, a website whose content in this case I’ve criticized earlier. However, instead of repeating myself I’ll state a few key points:
1) The benefits in primary prevention are naturally more modest than in secondary prevention. However, the “98% saw no benefit” should be placed in the proper context: these people wouldn’t have benefited in the first place as the vast majority of those in primary prevention don’t have a cardiac event during the five-year inspection period.
2) The key, however, is in understanding that a) we have to deal with preventing CVD on a population level and b) with the best possible kind of cure. Ideally, lifestyle intervention would be more than adequate – in fact, vastly superior to CVD medication due to a number of reasons. However, in real life that’s not the case.
3) Therefore, not using the best possible treatment in primary prevention would translate to a vast number of cardiac events in a primary prevention population as big as e.g. in the States. Therefore, in high risk population, statin treatment is the best option in primary prevention.
BTW, I’ve also criticized Roberts’ claim of women not benefiting at all. Which isn’t really the case.
Mie.
With regards to your comment on the association between cholesterol levels and mortality among the elderly, this recently published Japanese study may be worth looking at; https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3928456/
As in previous studies there was an inverse correlation between cholesterol/LDL-cholesterol and total mortality, and interestingly no correlation between cholesterol/LDL-cholesterol and death from cardiovascular causes.
So, is it possible that LDL-cholesterol becomes a weaker marker of risk as we get older? In fact I think that may be the case. Framingham data indicates that cholesterol is a much stronger risk factor before the age of fifty than later in life.
This makes sense to me!
There was a recent study on weight-bearing exercise for older men. An unexpected result: weight-bearing exercise raised their LDL levels.
I’ve also noticed that older people who exercise a lot are more likely to collapse under statins. Some of us imagine that this is because most of our LDL is “good” large fluffy LDL and is needed.
Before submitting to a statin, I asked if there was a test to analyze my LDLs, and my cardiologist said that “the science isn’t there yet”. Not correct, of course.
Most of us damaged older athletes have great triglyceride/HDL ratios and also HDL/LDL ratios. Even now, when I can almost not use my legs and am in constant significant pain from myopathy, I can run my pulse on an arm bicycle at 90% for 40 minutes, stop, and in one minute my pulse drops from 135 to 115 or lower.
I’ve never meant to say that statins may not help some people. What I’m saying is that almost no one knows about the 10-20% adverse effect level. And it seems to me, only a very, very small group of doctors and patients know about the extreme horrors, like mine and that of other people I’ve come to know…including, sadly, a cardiologist from the same group who prescribed to me.
Axel,
“With regards to your comment on the association between cholesterol levels and mortality among the elderly, this recently published Japanese study may be worth looking at; ”
I’ve read the paper earlier, but thanks anyway.
“So, is it possible that LDL-cholesterol becomes a weaker marker of risk as we get older?”
Well, I already kinda stated this. At this point (from what we know), it’s due to inverse correlation.
From your second article, which I can only partially access:
“…whereas the benefits of these drugs in elderly subjects without previous CV events are still debated.” Amazing that it’s still being debated after all these years, and yet what % of the elderly are on statins? 70% is my intuitive guess.
“In contrast, the risk of all-cause death (RR: 0.941 [95% CI: 0.856 to 1.035]; p = 0.210) and of CV death (RR: 0.907 [95% CI: 0.686 to 1.199]; p = 0.493) were not significantly reduced.”
And mortality not reduced.
And lord knows what happens to the 10% with muscle damage, etc? (Well, actually, I know too.)
And why always relative numbers when describing benefits?
This isn’t my field, so I make errors, but this is accurate from the Jupiter study: Fatal myocardial infarction was 50% higher for those on the statin vs the placebo group.
howfussiner,
“Amazing that it’s still being debated after all these years, and yet what % of the elderly are on statins? 70% is my intuitive guess.”
Yes, it is a bit amazing in my opinion too if we’re talking about CVD patient/people at a hight risk of CVD who started statin therapy before e.g. reaching 70 – although I find it amazing in a different way than you. When talking about initiating statin therapy in e.g. 70+ primary prevention patients with smaller risk, then it’s a different story.
“And mortality not reduced.”
Err, I kinda know (I linked the study, remember?). The point was that EVEN low risk population sees benefits.
“And lord knows what happens to the 10% with muscle damage, etc?”
10% get muscle PAIN. Myopathy vs myalgia?
And why always relative numbers when describing benefits?
“This isn’t my field, so I make errors, but this is accurate from the Jupiter study: Fatal myocardial infarction was 50% higher for those on the statin vs the placebo group.”
Ah, the “9 vs 6” question. Considering that the treatment group had the OVERALL mortality significantly reduced, this is hardly a problem if and when the idea is the reduce MORTALITY and/or cardiac events in general.
howfussiner,
“I’m trying to stay away from simplistic inflammatory statements.”
Then you’re doing a crappy job. By stating that funding is a disqualifying factor in RCTs, you’re de facto stating the “Big Pharma” mumbo jumbo.
“People who’ve already experienced a cardiovascular event may very well benefit from statins. I don’t know, and I don’t need to know.”
Please, you’re being intellectually dishonest here. For a person who “doesn’t know” whether people with established CVD benefit from statins or not, you’re quick to dismiss their benefits all around.
“Does this really surprise you?”
Err, read my answer. Hint: I wrote that I know this.
“The recent “expert” panel, in setting guidelines for statin use, raised the number on statins form the present 25% to a recommended over 40%. Many on the panel have ties to the pharmaceutical industry. Obviously only a fraction of the 40% have had a cardiovascular event.”
1. No need to use quotation marks, they indeed are experts in their field. Of course, experts too can be wrong but …
2. … this needs to be proven. Implying this and that about ties and funding don’t prove it. Valid criticism of the guidelines will.
“Actually that “something is going on” is evident from the studies themselves.”
Well then, let’s hear of a large statin trial that is obviously faulty. Go on.
“You know what relative numbers vs NNT are, no?”
Err … Why the “vs”?
“Research used to be funded my the NIH, which I think is a good idea.”
Please, do tell where the NIH would get the funding for X number of on-going drug trials. Their budget would increase enormously. Not to mention the financial risks that are now on the drug companies.
Go on. I’m listening.
By stating that funding is a disqualifying factor in RCTs, you’re de facto stating the “Big Pharma” mumbo jumbo.
This, of course, is not what I said. I simply said that studies funded by “Big Pharma” are 5 times more likely to reach conclusions favorable to “Big Pharma”. Harvard School of Public Health.
“whether people with established CVD benefit from statins or not, you’re quick to dismiss their benefits all around.
Also not what I said. If I were “dismissing their benefits all around”, I wouldn’t make a possible exception for people with established CVD.
What I’m saying is that the adverse effects of statins are hugely underreported, both as to number and severity. And I’m saying that statins are hugely over-prescribed.
Again, I don’t know what dog you have in this fight, but it feels to me like you’ve got one. The Harvard study applies to us as individuals as well, in a sense.
I never suggest to someone with established CVD that they go off statins.
But I certainly tell the millions of others about the risks/rewards.
Almost everyone I know who takes statins does so to get their LDLs down below the “ideal” of 100. And yet the “expert” panel has put the LDL number at 190 before recommending statins.
So….no conflict between us perhaps? Statins are not risk-free. Actually, for some people they bring horrible neuropathy, myopathy, and other nasty adverse effects.
So if we advice people whose LDL level is below 190 to revisit the issue under the new expert LDL guidelines, sounds like a good thing, no?
howfussiner,
“This, of course, is not what I said.”
C’mon, a little honesty please. If funding isn’t a disqualifying factor in your opinion, you wouldn’t have brought it up, right?
“Also not what I said. If I were “dismissing their benefits all around”, I wouldn’t make a possible exception for people with established CVD.”
So, calling statins “dangerous” and stating things like “LDL is just a number” is irrelevant too?
May I kindly suggest that you work on your written communication skills then?
“What I’m saying is that the adverse effects of statins are hugely underreported, both as to number and severity. And I’m saying that statins are hugely over-prescribed.”
Underreported, quite probably. But “hugely”? Cf. this study on statin-induced myopathy
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2517983/
16,7% of non-statins users vs 22% of statin users = not a “huge” difference. Of course, that’s just one study but still …
“Again, I don’t know what dog you have in this fight, but it feels to me like you’ve got one.”
Sure. I’m all for balanced reporting and discussion.
“So….no conflict between us perhaps? Statins are not risk-free.”
Well, there obviously is some even though you seem to try to step towards moderate from your initial claims. And of course: NO form of medication comes without side effects, that should go without saying.
“C’mon a little honesty please?” “May I kindly suggest that you work on your written communication skills?”
Sarcasm is lower on the scale than any honest attempt at communication, as inarticulate as it may ring to your particular ears. (You might also wonder if “pearls to swine” comes into the formula: I don’t think any level of communication skill could touch you.)
Now why is that?:
“It is difficult to get a man to understand something, when his salary depends upon his not understanding it!” Sinclaire
If it’s not salary, then what is it that causes your language to be so unrelentingly harsh to someone who has personally suffered a horrid adverse effect from a statin drug?
Last time: I’m not trying to get statins taken off the market, though to my understanding they are massively over-prescribed: the same AHA, ACC panel has recently changed its guidelines hugely. Even strong supporters of statin use exclaim that the numbers have been made up out of the air. I agree, but that’s not the point.
Again, last time: I’m writing because the adverse effects of statins are massively under-reported. I’m one of the many victims of this fact.
In my own case, statins did me in in six months. When I called the prescribing cardiologist, he said, “You have a serious disease, but it has nothing to do with statins.” I asked him what disease I had. He said that he didn’t know.
So I asked him how then he could know with such certainty that it wasn’t an adverse effect of statins.
Believe me, I’m anything but alone in this situation. Can you for a moment imagine where this leaves you?
Finally an advantage of aging! 😉
“Rough numbers (I’m happy to be fine-tuned): say 1 million or even 2 million US people have had a cardiac vascular event; about 32 million are on statins. (These numbers aren’t wildly off.)”
Source? According to e.g. this
https://circ.ahajournals.org/content/123/4/e18.full?ijkey=6afa2a66054600d558de39059f5f5af7df0b9f57&keytype2=tf_ipsecsha
more than a million people suffer an acute coronary event every year. Nearly 500 000 suffer a recurrent event every year. Surely that translates to more than 1-2 million having had a cardiac event once in their lives?
In addition, it’s estimated that as many as 80 million people in the States have some form of heart disease.
https://www.theheartfoundation.org/heart-disease-facts/heart-disease-statistics/
So yes, I’d also be interested to hear where you’ve gotten the idea that 95% of Americans taking statins means ANYTHING as it sure as hell doesn’t mean that these 95% are those who aren’t likely to benefit from statin therapy.
You know who I am: I’m an individual whose life has been massively altered by simvastatin, low-dose, taken for 7 months. I have severe myopathy in my legs: painful, debilitating, permanent. Want photographs, in case you think it’s myalgia? My legs look like the victim of a concentration camp. (My arms, however, are now impressively strong, since I’ve been reduced to working out on an arm bicycle.)
Before simvastatin I was on a great diet, was very physically active for 10-15 hours a week, and felt wonderful. I was grateful.
My doctors pushed and pushed statins because my LDL’s were “high”: I put that in quotes because the number for statin prescription has been raised to 190–by the “expert” panel of AHA, ACC. Too late for me.
I called the AHA before taking statins (actually I started with CDC who referred me to AHA, saying that’s where they got their information). I asked AHA, three separate phone calls, if I should take a statin: the information seemed to be contradictory and thus confusing to me as follows:
HDL/LDL ratio superb; trigliceride/HDL ratio superb; weight perfect; exercise perfect; LDL of 185. Everything except LDL tells us I’m really healthy.
Response: LDL 185? Take statin.
AHA recommended foods (their lucrative Seal of Approval) with trans fats until recently. Weren’t trans fats banned in Europe 10 or more years ago?
No, AHA is not an entity that I trust at all. I’ve just given a couple of reasons–things that have touched me personally.
Now what is it that you don’t trust about NNT and why?
And as I’ve asked before, what dog do you have in this fight? Me? I got wrecked by a drug that doctor after doctor told me afterwards that I never needed and that they never prescribe because of the percentage and the severity of adverse effects.
What I want is for my case to at least be reported as an adverse effect and thus become part of the data. Why do so many doctors resist doing this, do you think?
Enough. Without knowing your agenda, what you want, I have no way to know if you’re part of the statin industry or exactly what you are.
What I do know is that you use strong and insulting language, so you must have something going on.
Its a pity a few of you cant get off your soap boxes and every time someone comes on here and mentions statins, it turns into a frenzy of posts about statins and its the same old arguments weve heard a thousand times. Your offering nothing constructive to the original posters, so please take your arguments somewhere else, you sound like broken records ans youre ruining it for everyone else!
howfussiner,
“Again, last time: I’m writing because the adverse effects of statins are massively under-reported. I’m one of the many victims of this fact.”
No need to repeat yourself. My “problem” is not this but … Well, read my replies.
“Without knowing your agenda, what you want, I have no way to know if you’re part of the statin industry or exactly what you are. What I do know is that you use strong and insulting language, so you must have something going on.”
Well well, surprise surprise. Point out inaccuracies and blatantly biased claims –> you’re part of Big Pharma. Yep.
This may come as a surprise to you but the truth/information value of a statement DOES NOT depend on the person saying it.
Now, as for my language: it is what it is mostly due to the fact that once you see the same erroneous claims repeated for the n:th time, it’s not exactly a pleasure anymore.
However, please refer to where and how I’ve “insulted” you? The “little honesty here” part? That was justified, given what you wrote. “Strong language”? Yes, I used the word “hell”. So?
And one more thing: I personally would prefer you comment on the information I’ve provided concerning e.g. the prevalence of side effects, the efficacy in primary prevention etc. etc. That should be the primary concern here, not hurt feelings.
I’ve read what you wrote and humbly disagree with a good deal of it for factual reasons.
But as Sinclaire expressed so well…. I frankly have no idea who you are or what your motives are. So you can remain the mysterious expert. Have you ever heard of “Professor Cory, World’s Greatest Expert”? At least we all knew that he was a comedian.
You may disagree, but if one cannot defend one’s opinions in fact-based discussion then – normally – a person should realize that the opinions weren’t worth defending in the first place (that is, they were in error).
Ad persona is a waste of time.
My opinion is that the adverse effects of statins are hugely unreported. Also that statins are hugely overprescribed.
I don’t know why you feel that these things are attack/defend issues.
The question of over-prescription is addressed indirectly in Dr S’s discussion elsewhere of more predictive indicators than LDL-C for future cardiovascular disease. I’ve mentioned Triglycerides/HDL, for example; and LDL/HDL.
And there are dietary and exercise means of changing these numbers for the better. As we age, diet and exercise may not keep LDL-C in numbers that some doctors want. But if the other numbers are excellent, if weight is correct, and if one exercises, is the risk of statin adverse effects worth it?
Amen!
howfussiner,
“My opinion is that the adverse effects of statins are hugely unreported. Also that statins are hugely overprescribed.”
Oh really? 🙂 As I’ve pointed out – and will point out here for the final time – these kind of statements aren’t opinions per se but factual statements which of course require data to back them up.
So fat that part’s lacking and/or faulty (as the withdrawn Abramson) in your replies.
“The question of over-prescription is addressed indirectly in Dr S’s discussion elsewhere of more predictive indicators than LDL-C for future cardiovascular disease”
Err, you’re confusing risk indicators with the best current form of treatment.
We disagree on the “best current form of treatment”. Diet, exercise, weight control, etc. are certainly the best. (That’s not fair of me to say, because my guess is that you also feel this way.)
At a recent phlebotomist visit, the woman drawing blood told me that her son was prescribed a statin for high cholesterol. She told the doctor no, that first she was going to more carefully examine his diet. Her son is 7 years old. Seven.
Yes, statins seem to be the only medication that lowers LDL-C. But they are not without possible horrible and permanent adverse effects. Agreed?
I sent you NNT numbers which you dismissed out of hand. You also said you disagreed with Dr Roberts, Cardiologist. And you said that you didn’t “like” that NNT site. With all due respect, that doesn’t move discussion forward. You may very well have good reason to doubt the NNT website, and if so, I will open-mindedly hear them out.
You are right to point out the real emanating of that 9/6 actual number vs the relative 50% relative number on my Jupiter Study example. In fact, that was my point. Relative numbers are pretty much meaningless–but very often used in medication sales pitches. (Although if the study hadn’t been stopped early, the 9/6 might have looked different in the end, who knows?) Very often the benefits of a medication are expressed in relative terms, and the adverse effects in % of those who take the drug.
Made up example: 52% lower CVD. 1.6% get diabetes. Comparing these numbers makes no sense, of course. But the first one sure looks bigger!
By the way, I’ve seen three cardiologists after taking statins for six months. All three of them independently said that before statin, I was at very low risk for CVD.
Just because we have only one medication, it doesn’t logically mean that it should be used so much. There is ongoing debate about what particular combinations of things predict CVD. What strikes me is this: after all this time, there is a great deal of disagreement. One would think that if 25% and higher of Americans over 40 are being medicated, that after 40 years or so, there wouldn’t be so many MDs, research scientists, etc in debate about the predictors and also the dangers and efficacy of the medication.
howfussiner,
“Diet, exercise, weight control, etc. are certainly the best.”
Correction: they WOULD be the best. If people in general could follow these guidelines. However, they cannot. See e.g. this meta-analysis on different options for CVD treatment and mortality
https://www.ncbi.nlm.nih.gov/pubmed/15824290
Dietary interventions as a whole don’t have a statistically significant effect.
“But they are not without possible horrible and permanent adverse effects. Agreed?”
Can you not read? I already answered this! The serious side effects are, however, very rare and benefits are much greater in high risk population.
Concerning Roberts and NNT.com: I already mentioned having dealth with them before. Now, unlike you, I dislike having to repeat myself. See here for Roberts:
https://www.docsopinion.com/2013/06/24/heart-disease-and-statins-do-women-differ-from-men/
I also made comments why I consider NNT.com’s estimate in primary prevention somewhat inaccurate. I’ve commented on them too here (and elsewhere), including the mismatch between the most recent Cochrane review (Taylor et al, ”Statins for the primary prevention of cardiovascular disease ”), the failure to differentiate the differences in effects in different study populations (many primary prevention studies conducted, at least partially, among individuals with less risk of CVD; newer studies conducted outside the “core groups”), the lack of differentiating between the nature of adverse effects in terms of NNH etc.
“Relative numbers are pretty much meaningless–but very often used in medication sales pitches.”
Wrong. Of course they aren’t “meaningless”: given the nature and prevalence of CVD, we’re talking about the difference of thousands of lives saved and cardiac events avoided on a population level. But naturally, when considering whether to treat an individual and how to treat them, the solution is done based on absolute risk.
“What strikes me is this: after all this time, there is a great deal of disagreement.”
What strikes me is the fact that you seem to have no idea of medicine and science in general. There’s always disagreement to some extent. However, what matters is the evidence – and in the case of statins, it’s solid when it comes to sc. “core groups” who to treat. E.g. guidelines around the world are unanimous in the basics. And they aren’t exactly anything but conservative.
Hi Doc, I.m 48 years old, female, 5.8, 142 lbs, non smoker, around 7 alcohol drinks a week, exercise 3x/week, health eater, normal blood pressure, have mild heart murmur, vitamin D always low for which I take 1,000 i.u. every day. My lipoprofile test:
LDL-C: 148
Total Cholesterol: 229
HDL-C: 58
Triglycerides: 117
LDL-P: 1930
Small LDL-P: 387
LDL size: 21.9 (nm)
HDL size: 9.0 (nm)
Family history of high blood pressure (mother, sisters), high cholesterol, borderline diabetes (mother), but most of my mother’s issues resolved when she lost weight, family overweight.
The question is that my doctor is insisting that I take statins saying that I’m at high risk of a heart problem specially because of the high LDL-P numbers. Is it true? Can I try something else, like niacin? Does niacin really work?
Thank you very much /
@ Edna
Statins may to some extent reduce the risk of heart attack and stroke in healthy individuals with increased risk. However, the effect seems smaller among women and men and there is no clear evidence of that these drugs lower mortality among women in primary prevention.
No other drugs have been shown to reduce risk to the same extent as statins do. Niacin will certainly improve your lipid numbers, but there is very limited evidence for a clinical benefit.
There is always some risk of adverse effects of statins although most people appear to tolerate them well. There is no doubt your lipid numbers will improve on statins.
The question whether to treat or not with statins in primary prevention can be a difficult one. Of course your LDL-P is quite high. However, it is important to see the whole picture. To me your general risk appears quite low. In fact there are risk calculators that can be used to asses risk.
So, it all comes down to shared decision making between you and your doctor. Do the risks outweigh the proposed benefits? I probably wouldn’t push it very hard if you were my patient. Also remember that lifestyle measures weigh strongly.
Thank you so much for your reply, I think I’m not going to take statins for a bit longer because I’m not sure if it’s the best approach. I should exercise more, eat less carbs and stop the alcohol altogether.
Can you not read? I already answered this! The serious side effects are, however, very rare and benefits are much greater in high risk population. (You don’t and can’t know this: adverse effects are underreported. I know of no one, including myself, whose doctor reported the adverse effect.)
What strikes me is the fact that you seem to have no idea of medicine and science in general. (Would you like to compare academic credentials? But it doesn’t require academic credentials to treat others with respect.)
If people in general could follow these guidelines. (Exactly this “people in general” is a major criticism of present medicine. Just because if every single person in the world took statin, the numbers might improve, that doesn’t logically mean that it would be a sensible protocol. Not even if the overall numbers did improve.)
Wrong. Of course they aren’t “meaningless”: given the nature and prevalence of CVD, we’re talking about the difference of thousands of lives saved and cardiac events avoided on a population level. (Using relative percentages for positive events and absolute numbers for adverse effects is dishonest: you know the old adage about statistics, of course.)
howfussiner,
“You don’t and can’t know this: adverse effects are underreported.”
Presuming you’re still talking about SERIOUS side effects: so you say. I have no intention of taking just your word for it. Cite studies INDICATING the magnitude of the effect, please. The aforementioned Abramson et al was withdrawn so don’t bother with it.
“But it doesn’t require academic credentials to treat others with respect.”
I prioritize arguments, you moan about respect. Guess which one of us is better equipped for a FACT-BASED discussion?
“Exactly this “people in general” is a major criticism of present medicine. Just because if every single person in the world took statin, the numbers might improve, that doesn’t logically mean that it would be a sensible protocol. Not even if the overall numbers did improve.”
You’re making absolutely no sense here. Of course you’re not going to treat each and every individual but those shown to be likely to benefit. When considering what approach to take, you do so based on EVIDENCE from clinical studies and epidemiological studies (follow-ups).
“Using relative percentages for positive events and absolute numbers for adverse effects is dishonest: you know the old adage about statistics, of course.”
Since absolute benefits outweigh the absolute harms, your point is meaningless. E.g. in high risk primary prevention far more people are spared from a cardiac event than get serious side effect. For instance rhabdomyolysis (probably the most serious side effect of statin therapy): its prevalence is 3-4 cases per 100 000 person-years of statin treatment and at least partially due to e.g. problems with other pre-existing medication, medical conditions such as CKD. Compare that to the reduction in cardiac events which is considerably bigger in the same number of person-years.
Thank you. If my doctor had provided information of this quality, it would have saved my health. I would never have taken simvastatin.
I feel like I’m in touch with… Well, you remember the Sinclair quote, no? What motivates you, I sincerely wonder. Or are you perhaps a Tea Party radio talk show host?
Just having strong opinions and insulting others doesn’t mean that you’re right–or for that matter that you’re wrong. It just leads to no further knowledge to anyone.
Frankly, although you have a lot of facts floating around, it’s impossible to engage you in a discussion with any movement. You’re always on the attack against things you don’t believe already or defending the things you already do believe.
I don’t want to be involved in a fruitless, circular insult competition.
You’ve been helpful to me in tweaking a few things that I was going to send on postcards that some of us send to the doctors who prescribed statins to us. These are the doctors who refuse to report consequent adverse effects to the FDA. (The other side of the postcards have photos showing severe myopathies which occurred within months of taking statins.) So thank you for dotting a couple of i’s for us.
Adios
PS Yes, I’m sure you’ll say, “I won! I won!” What’s the prize?
Next time less martyrdom and pathos, please.
Hello,
I am a vegetarian, and get cardio in for 30 min 5-7 times per week. I am on 10mg Lipitor and 5mg amlodipine. Cholesterol and bp are controlled. Mother’s side of family has high cholesterol and BP. My recent results:
Cholesterol =160
LDL-C = 91
HDL-C = 53
LDL -P = 1609
Triglycerides = 81
Small LDL-P = 974
HDL-P (total) = 35.7
LDL Size= 20.5
VLDL Size = 39.1
Large HDL-P = 4.1
Large VLDL-P = 0.8
I do eat a lot of carbs as a vegetarian, but have started a planted based diet (no more diary and eggs). I am 5ft 8in and weigh 147lb, and 40 years old. We also have diabetes in on both side of the family. My parents don’t have high cholesterol, BP, or diabetes though.
Thoughts on what to do bc I am frustrated…Thank you!
I took Simvastatin for close to 5 years–the lowest dose possible (10 mg) daily). My total cholesterol was in the 190s.
Because I am suspicious regarding statins being over prescribed and because of what they do to one’s liver (and other side affects), I stopped altogether two months ago.
My diet is mostly protein and veggies, low (but not no) carb.
I exercise a lot at least 5 times weekly.
I am 5’11” and weigh 198 lbs.
Recent NMR LipoProfile says my LDL-P is 1869 HIGH.
My LDL-C is 151 HIGH
Total Cholestrol is 225 (which is high by standard opinion, but I have been led to believe that total under 275 is okay?)
HDL-P (Total) 34.9 What does this mean?
Small LDL-P 340 What does this mean?
LDL Size 21.0 What does this mean?
After 25 years with a major prescription drug prescribing HMO, I am without insurance and am looking for a Doctor who is not obsessed with low cholestrol and prescribing statins. How do I find that?
Thanks
———————————————————-
Seek out integrative MD, I will see only integrative types….those conventional MD’s….get more and more arthritis of the wrist from writing scripts day in and day out…….
My integrative MD is more concerned about homocysteine and since mine was getting higher I’m taking supps to get it down…..do some work on homocysteine and the heart….there is a ton of info on this issue……cholesterol drugs are HUGE money makers for pharma…..grrrrrrrrrr
Huge money-makers and for some people devastatingly dangerous. Statins can cause permanent neuromuscular diseases. And note: the “expert” panel from AHA and AAC has just raised the LDL level to 190 for statin to be indicated.
So … When you get exposed for spreading unsubstantiated claims, you just … Leave with pathos and return a couple of weeks later as if nothing happened?
Seriously. Please. 🙂
Dr Sigurdsson is such a doctor, I believe. You may know that the new “expert” guideline for statin prescription is LDL at 190 or over: so you’re already “cured”. (AHA and AAC released their new panel’s guidelines late last year.) And you should know that for some people statins can trigger lifetime, devastating neuromuscular diseases. I am one of these people, and I know of thousands of others.
There are many ways to better predict CVD than LDL-C. You will find them here: i.e. Dr S’s discussion of tri/HDL ratio.
But the only drug that Big Pharma has is statins–which simply lower LDL-C: there’s $30 billion in business pushing for more statin use. Keep your money and most importantly your health!
Question: where did you get your lipid profile done? I’m in the USA, and my PCP isn’t even familiar with some of the data you provide. I ask because I’d like to get a meaningful test done myself. Thank you.
I have always had high cholesterol but only recently I was able to convince my doctor to do an actual measured (rather than calculated) test of my LDL. The results are perplexing.
My total cholesterol is 336
HDL-C is 67
HDL-P is 32.1
LDL-C is 257
LDL-P is a staggering 3411
However, triglycerides are only 62
I also had a coronary calcium scan done. Score was zero (0). No calcification.
My CRP levels are elevated at 3.21, indicating inflammation. I also have chronic pain and fatigue consistent with fibromyalgia symptoms. I also have chronic hypertension and have for about 30 years. It has been very difficult to control with drugs, and of the few that work, bizarre and debilitating side effects come with them. Same for statins. Almost no effect, very bad side effects.
I have been on many diets including vegan, vegetarian, low fat, Sugar Busters, Atkins, etc. Nothing had any significant impact on my cholesterol level except the low carb diets. Fours years ago I went paleo and lost a lot of weight and saw my triglycerides plummet from 135 to 54. But total cholesterol climbed a little, which isn’t unusual on paleo. Overall, my health and quality of live improved on paleo but I’m still, obviously, battling some serious, undefined issues. Doctor wants me to pursue Chronic Inflammatory Response Syndrome but little is known about it. Not sure if inflammation can cause such a high LDL-P number but I’m out of other ideas.
Forgot to mention, 50 y/o male. about 30 lbs. overweight but even when I was trim, I had the same problems. Non-smoker. Physical job, get a lot of exercise. No family history of coronary artery disease in anyone younger than 75. Have had relatives that have had cardiac events, but they were very old. Mother has similar issues to mine (chronic pain/fatigue [fibro], high BP, carb intolerance). But she is 73 and still going strong. I suspect that if I ever finds out what is driving this in me, I’ll solve her problems too. That is, IF there is even a treatment.
I also have chronic pain and fatigue consistent with fibromyalgia symptoms.
Did you have these problems before taking a statin drug, or only afterwards?
https://www.nytimes.com/2014/08/15/technology/web-trolls-winning-as-incivility-increases.html
I have had similar struggles. I now live on a Gluten-free and dairy-free diet, which for me lowers inflammation. I need to go back and get new blood levels drawn. Do you have any known auto-immune disorders or food allergies?
Forgot to mention, my diet is also low carb.
Dr. Thomas Dayspring MD looks like a rather unhealthy (read fat) specimen. Wonder what his numbers are.
I have been taking the Health Diagnostics Lab tests for several years. I went on a low carb (generally less than 50 net carbs/day) diet in Feb 2013 with very occasional splurges like french fries. Since that time most of my numbers have steadily improved. Now:
Total C = 180
LDL-C = 97
HDL-C = 72
Triglycerides = 79
What’s puzzling is my LDL-P which had dropped to 891 from 1418, and is now back to 1445.
I am Apolipoprotein E Type 3/4
Dr. Sigurdsson,
Even though I’m vegan, I just realized that my saturated fat intake, mostly from olive oil and nuts, is far higher than my carnivorous friends. At 2 grams a tablespoon, I probably get 12 grams a day from olive oil alone; in total, I may be as high as 25 grams a day from plant-based sources. Is a purely volumetric comparison of saturated fats from animal sources vs. plant sources fair in terms of heart risks? That said, my LDL-C is 128 (HDL 79; Trigs 55). I would like to lower it. Would reduced oil intake help?
Thanks much,
Russell Long, Ph.D.
Russel.
Different types of saturated fats may influence cholesterol somewhat differently. The effect is sometimes hard to predict and there may be individual differences. In your case I don’t believe you have to worry about saturated fatty acids from plant based sources.
In my opinion your lipid profile is fine. For example your non-HDL cholesterol is very good.
It is possible that reduced oil intake will lower your LDL cholesterol. But, that won’t necessarily improve your health.
So … You eat nearly 100 grams of olive oil (according to this,
https://www.fineli.fi/food.php?foodid=536
olive oil has about 14 g of SAFA per 100 g) a day? Seriously? And so much other plant-based fats that you get 12 g more, even though e.g. most nuts have only about 6 g of SAFA per 100 g meaning that you’d have to eat 200 g of nuts a day?
Seriously?
Hi doc.
Your comments did give a lot of info I was looking about cholesterol.
I just had a lipid profile test wherein LDL is in the ‘moderately high risk’ stage. HDL is at 42.
I had the lipid profile test after a 40 min brisk walk. Is it ok. or should I have a lipid profile test again.
@ Naveen.
No you shouldn’t need another test.
Hi,
I’m hoping you can provide some advice. I’m a 37 yo female, 175 lbs, 5’4″
Mom is type 2 diabetic, and has had 2 stints. Dad very healthy. Both grandmothers living, good overall health except fibromyalgia. Maternal grandfather died in 30’s from untreated diabetic complications, paternal grandpa died this year at 91.
Here’s my dilemma:
LDL P 2648
LDL SMALL P 1686
LDL C 152
HDL C 49
LDL SIZE 20.7
HDL P 28
TOTAL C 248
Triglycerides 237
LP IR 70
The only abnormality on blood work was low vitamin D, now 40.2 after weekly supplement. My MCV is slightly high 98. THS was normal, but somewhat high 3.21.
The kicker is I’m positive for B. Burgdorferi antibody, but negative western blot. Doctor recommended statin, but I declined until I could investigate. I was treated for RMSV last summer, after vasculitis in my legs and feet and ended up hospitalized for crippling headaches 3 days after antibiotics started. Took 30 days worth and still battling headaches & fatigue.
Does one have anything to do with the other? I have 2 young kids and really want to be around a while. Should I get a CT or ultrasound? PCP said my coronary artery sounds good, as does my heart. No angina either.
Thank you for your time.
Thank you.
Also, Glucose was 94. Sorry for leaving that out.
Hello Doc. I went to a weight loss clinic to begin the HCG diet. I’m 5’2″ and 160 lbs. They did preliminary labwork and I was amazed at my lab results. My cholesterol went from 165 in Jan 2014 to 286 currently (Aug 2014) In addition, my TSH was normal in January 2014. Currently, my TSH is 118, ldl-p 2137, lymphs 52.0, thyroxine (FT4) 0.11, and (FT3) 0.7. I had an US of my Thyroid about 3 weeks ago. I started on Amour 60mg daily and basically was sent on my way. I’m so worried I can hardly sleep. My cholesterol level have worried about my heart. In addition, I’ve been getting symptoms like Reynauds syndrome in my fingers. Should I be doing something?
Thanks for the post Garri.
I have no experience with the HCG diet and I know very little about it to be honest.
I wouldn’t recommend it to anyone unless I was convinced it doesn’t have any adverse health effects.
Wish you all the best and hope you’ll recover soon.
My total cholesterol level is 160. I am 42 years old. Weight train at least 4 days a week. Im 5’8″ and weigh 185. And I am a tobacco user. Do not know my other levels. Donated blood and they sent this information. I read one of your post above and it alarmed me. Do I have need to worry here? Also , I might add that I am not on a particular diet. I basically eat normal.
Hi Pat.
From what you wrote I can’t see anything you should have to worry about. Continue with your regular exercise and healthy eating habits. To me “eat normal” sounds good. You can eat healthy without being on a specific diet. Just enjoy being young and healthy, it never lasts forever.
Hello doc:
I am a vegetarian, and get cardio in for 30 min 5-7 times per week. I am on 10mg Lipitor and 5mg amlodipine. Cholesterol and bp are controlled. Mother’s side of family has high cholesterol and BP. My recent results:
Cholesterol =160
LDL-C = 91
HDL-C = 53
LDL -P = 1609
Triglycerides = 81
Small LDL-P = 974
HDL-P (total) = 35.7
LDL Size= 20.5
VLDL Size = 39.1
Large HDL-P = 4.1
Large VLDL-P = 0.8
I do eat a lot of carbs as a vegetarian, but have started a planted based diet (no more diary and eggs). I am 5ft 8in and weigh 147lb, and 40 years old. We also have diabetes in on both side of the family. My parents don’t have high cholesterol, BP, or diabetes though.
Thoughts on what to do bc I am frustrated…Thank you!
I assume the thing you are most concerned with is the LDL-P and the preponderance of small particles.
In your case, total cholesterol is probably nothing to worry about and LCL-C is not high. A TG/HDL ratio of less than to is not that bad either.
I believe you should focus on reducing your risk in genaeral rather than focusing on certain numbers. So not smoking, healthy eating and regular exercise are key factors. I assume your BP is taken care of, partly by the meds (amlodipine).
A plant base diet is generally considered beneficial with regards to the risk of heart disease. It usually lowers LDL-cholesterol and so of course does the atorvastatin (Lipitor). So I really can’t recommend that you don’t stick with that. Of course you should avoid sugar and refined carbs, I assume you do that already.
Of course LDL-C and LDL-P are partly genetically determined. In your case there seems to be some discordance (low LDL-C and high LDL-P). Without the Lipitor, LDL-C and LDL-P would both be higher. So stopping the drug will make your numbers worse.
I’m not sure if there’s any specific measure, apart from what you’re doing that might lower LDL-P further. Possibly you could try to reduce carbs and add fat. That might help lower LDL-P. You could still stick with your plant based diet if that’s what you prefer.
Maybe adding fish, fish oils and marine omega-3 fatty acids might help improving your numbers if that’s what your after.
Hi Doc I just got my fasting labs back in and it’s got me scared. I am 24 years old 5’11 and weight is 234 lbs
My total cholesterol is 161
LDL-C 94
HDL-C 29
Triglycerides 369
NON-HDL-C 132
Apo B 85
LDL-P 1784
sdLDL-C 40
% sdLDL-C 42
Apo A-I 95
HDL-P 20.9
HDL2-C 8
Apo B:Apo A-I ratio 0.90
Lp(a) Mass 10
Lp(a)-P <50
Both sides of my family have died from heart disease. All I was given to help was Lovastatin. Is there and other things I can use to help the Lovastatin?
David
You certainly fulfill criteria for the metabolic syndrome. BMI>30, high TG, low HDL cholesterol, probably visceral obesity. LDL-C not that bad but LDL-P high. That’s typical discordance.
Losing weight should be a primary target. Of course there are many ways to go. In my experience carbohydrate restriction often very effectively reverses many of the features of the metabolic syndrome. You can read more here.
Best of luck.
I have an LP-IR score of 75. What is my risk of type 2 diabetes.
Terry.
LP-IR score reflects insulin resistance. Higher score is associated with increased risk of type-2 diabetes. However, I don’t think it’s possible to exactly assess the risk of developing diabetes from the LP-IR score. Many other factors come in to play.
Hello sir.
my ldl cholesterol- direct is 78mg%. However it is written that the normal range is 85-130.
Is there something to be worried about..?
please fo reply.
Thank you.
LDL cholesterol 78 mg/dL is good, no worries.
I know this website presents quality dependent
posts and other stuff, is there any other website which offers these kinds
of things in quality?
That’s a great question! Do you mean specifically related to cardiovascular wellness? Along with high risk for CVD, I have auto-immune disease and a plethora of allergies, and I’d like to follow a blog such as this related to those problems.
There is an indepth discussion on heart disease on a forum that is specifically related to ApoE4 carriers, so they discuss many other conditions as well. But there is a lot of research members go into as well as self experimentation on different diets and how they affect lipid markers.
The main site is http://www.apoe4.info.
Like many before me I just got my numbers and am confused.
Non smoker
exercise 4-5 per week
went off statin drug about a year ago
recently lost 20 pounds
70 years old
Mother and brother and many cousins on mother’s side died of heart attack
Mother also had diabetes
try to eat no grains or sugar (slip once in a while)
taking citrus bergamonte
Numbers:
Total Cholesterol 238, down from 268 (yeah)
LDL-c 178
HDL-c 67
Triglycerides 118
Non HDL-C 171
Apo B 125
LDL-P 2453 (ugh)
sdLDL-C 43
Apo A-1 154
HDl_p 50
Hdl2-C 20
Apo B: ApoA-1 ration .81
Lp (a) P 137
Any suggestions….?
Yes,one bit of advice: stay off statins!!! I’m 71, and lost the ability to hike, bike, swim from statins about 2 years ago. Permanent myopathy. Constant pain.
Dear Doctor Sigurdsson,
I’m concerned because my recent NMR shows my LDL-P jumping from 366 to 1320 in 17 months.
some history
– family history of early heart disease
– age 68 – 5’3” – 100 lbs – BP 110/70
– daily exercise; super healthy low carb diet with minimal processed foods and sugars
– glucose range – 95-100; post prandial readings are high – hence the focus on very low carbs
– 2007 heart scan = 207; 2008 heart scan = 260
(my older brother’s heart scan was1600 at age 67)
– initial treatment – 20mg vytorin for 1 month resulted in thigh pain which took 5 yrs to resolve
– niacin worked well to reduce LDL-p; however due to elevated ast/alt, niacin was cut to 500mg.
8/2007 12/2007 6/2013 11/2014
LDL-P 1033 401 366 1320
LDL small 328 67 <90 188
trig 50 44 31 56
HDL 73 78 101 120
niacin mg — 1000 1000 500
Based on my now normal ast/alt and the increased LDL-p, I’ve increased my niacin to 1500mg and will retest both the NMR and ast/alt in 3 months.
Niacin’s gotten some negative press recently but it is my understanding that the AIM – high study tested niacin as an additive to statin therapy. And the HPS- thrive study included laropiprant which may have skewed the results.
What are your thoughts re my increasing my niacin to attack the LDL-p?
In your experience, is it unusual to have such a large increase in LDL-p in short a short time span?
thank you!
i have high blood sugar, ldl cholesterol and triglycerides, can i eat raw avacado
I just woke up to Dr. David Perlmutter on the importance of Good Fats…which includes avacodo, coconut oil and oilive oil and the need for cholesterol….he wrote the Grain Brain which I find fascinating…..get the grains and carbs/sugars out of your lives….
It’s an old article, but it got me interested. I am a 55 year old female, normal sugar, normal blood pressure (without drugs), high normal weight (131 pounds, 5’2″), never smoker. Both of my parents had high cholesterol and both were/are on statins; mother had blood pressure, but she was also very overweight, borderline-obese. Father *may* have had a heart attack sometime between ages 50 and 60: he’s never noticed it, the doctor who looked at his EKG at 60 told it showed heart attack, his previous EKG was at some point after 50. Anyway, I just got a call from my primary care after check up, my total cholesterol is 264, LDL – 191, HDL-59, triglecerides – 63. He’s never mentioned LDL-C vs LDL-P – I suspect it wasn’t even checked. He suggests trying lifestyle measures for 3 months then consider statins if it doesn’t work. I do plan to lose 5-8 pounds or so and exercise more. My fear is that given that I am not particularly overweight, I am not sure how much effect lifestyle changes would have. I am even more reluctant to take statins given that I think my absolute risk even with this high LDL is still fairly low. I wish I knew LDL-C vs LDL-P, but I don’t have these numbers.
Hi Kitty
LDL-C is calculated from the other numbers (LDL-C = 264 – 59- 63/5 = 193). So your LDL-C is approx. 193.
You’ll need a special analysis for LDL-P so that’s probably not been checked.
I´m quite sure you can lower your LDL-C by lifestyle measures.
Thank you. Appreciate the reply, gives me hope increasing exercise and losing a few pounds will work.
OK, so 3 months went by and I had another test, and it’s strange. My total cholesterol and LDL-C are both down to 214 and 155 respectively, but my triglycerides are 74 and my HDL dropped to 47 which is a mystery to me. During this time I lost 13 pounds (120 pounds now – if I lose much more, I’ll be anorexic), increased exercise considerably, and made very little changes to the diet except for maybe increasing fish relative to meat/poultry a little; increased nuts making some other portions smaller in exchange, replaced some of the grain side dishes with vegetable, decreased sugar and reduced total calories a little – nothing drastic, fairly small changes, I am not into junk food. From the exercise perspective I went from being mostly sedentary and only walking on weekends to exercising every day for an hour, something aerobic like either very brisk walking and zumba on 5 days a week and strength training on the other two days). So in total, I exercise at least 7 hours a week, usually spending 300-500 calories each time. So why is my HDL down so much and my ratios are worse? Doesn’t seem to make any sense to me.
You should know that for some people statins can cause permanent devastating neuromuscular diseases. The overall adverse effect percentage is about 10%. If your physician isn’t aware of these facts, you should make your decision with a physician who is aware of the potential downsides.
Merry Christmas, Doc! Thanks for giving us information and hope in or cholesterol-ridden lives!
Thanks Katy. Merry Christmas.
I have Kaiser and I can’t get a break down of cholesterol past this, and nobody else will give me a blood test since I have Kaiser. My total cholesterol was 250, Trigycerides 52, HDL 62 and LDL was178. The only thing that works for me is STATINS, but then I started coming up prediabetic. I think the Statins caused it. I have no family history of diabetes. I weigh 124 pounds and am 5 foot 2 and exercise and eat a diabetic diet. (fill your plate method) 1/2 veggies, side of fruit 1/4 plate protein, 1/4 plate carbohydrate. My mom and dad had heart disease. I am 49. I know the doctor is going to want to put me on Statins AGAIN! I hate STatins, They also caused muscle cramps and muscle pain. (I never had the “prediabetic” problem before taking Statins) I do have a family history of hypercholesterolemia. (my mom has that) My dad never had that, but still had heart disease. My mom took statins and it did not prevent the first heart attack anyway. I am trying some supplements to get that LDL down, but nothing ever works. Any advice??
For Lucy…. have you ever read all the info and even books on the Cholesterol Myth…… my integrative MD is not concerned about cholesterol so much, it’s homocysteine and the heart…..read The Heart Revolution. Those statins are deadly and a big profit hog for pharma….
Read Weston Price info on cholesterol and oils in general.
Strong advice: stay away from the statins. Your triglyceride/HDL ratio is great and is a better predictor of heart disease. In my case, even ignoring the positives of good diet and tons of exercise (which would make the difference even smaller), if I’d lowered my LDL from 196 to 100, it would change my risk of heart disease from 10% to 8% over the next ten years (taking me to age 78) according to NIH. Not worth it!
What happened is that I took 20 mg simvastatin for 6 months and got a not uncommon autoimmune reaction. Now I can’t walk, my leg muscles have visibly rotted off, I got a blood clot almost immediately, etc. etc. This is so common that one of the doctors in the cardiological group has had the same terrible experience. Neither of our cases has been reported by the prescribing physicians.
As one of the many victims, I wholeheartedly agree. The adverse effects, well-documented, are seemingly unending. For example, a new one that many of us are experiencing is a strange skin rash. (Note that “rare” means “reported rarely”.)
A patient developed an adult-onset dermatomyositis-like syndrome characterized by skin rash and progressive proximal muscle weakness concurrent with the intake of simvastatin. Despite discontinuation of the statin, symptoms progressed and required conventional steroid therapy for remission. The association between statins and the development of a musculocutaneous syndrome closely resembling dermatomyositis in susceptible subjects is poorly understood and has been reported rarely. The purpose of this report is to provide additional support for this pathological association. Since the population receiving statins is large and rapidly growing, caregivers are urged to be alert regarding the early recognition and proper care of the spectrum of neuromuscular complications linked to statin intake.
For Joy, I did read that book Cholesterol Myth a few months ago. So far I am disgusted and I don’t want anything to do with Statins.(I think they gave me pre diabetes) I think the doctors underplay their side effects. The only oil I use is olive oil. All I have left is waiting for the signs of a heart attack and hoping the big one doesn’t get me, before I can get stents or something.
@ Joy I forgot to mention. I did that inflammation test and my inflammation is low. Thanks for the advice. I guess, I’ll take my chances and hope for the best.
@Lucy – I found this website (one doctor’s blog had a link), it looks really good in showing exactly how much benefit vs risk one can get from statin:
https://www.thennt.com/nnt/statins-for-heart-disease-prevention-without-prior-heart-disease/
You can click on “Customize This NNT” in the blue box on the right, enter your own numbers and see number needed to treat to get benefit and also to suffer harms as related to your specific case. Always remember – the issue isn’t pleasing your doctor or getting the right number, but how you feel about benefit for you personally in terms of absolute risk reduction vs risk of harms.
Also read Peter Gøtzsche’s latest book ‘Deadly Medicines and Organised Crime: How Big Pharma has Corrupted Healthcare’ wins first prize in BMA book awards 2014. (BMA is the British Medical Association.)
I like this site, but it still uses the statin-promoting relative number rather than the absolute number. For me, for example, it says, “Statins reduce your cardiac risk by about 25%” This is almost meaningless. What is really the case is that it takes my risk from 9.9% to 7.4%…at best. That’s 1.5% less heart disease by any normal person’s reading of statistics.
(Again, exercise, weight, triglycerides, etc are not factored in.)
You didn’t use ‘reply’ so I am not sure if you refer to the NNT calculation link I referenced or something else. The whole point of this site is that while it mentions the relative risk reduction, it actually recalculates it in terms of NNT/absolute risk reduction for your case. Sure the first line is about 25%, but if you read the explanation below and enter your numbers, it recalculates your absolute risk reduction and shows it graphically. For me, the numbers are even smaller than yours — 0.4% reduction in relative numbers. Sure, it doesn’t factor in weight or exercise or TC, but it’s still a good approximation.
I am using “reply”, but not sure it’s working right. I understand what you’re saying, and I do like NNT. But I still feel that we should all avoid EVER using relative numbers in the way the 25% was used. It’s Big Pharma’s way of selling drugs: put the upside in a relative number (25% yay!) and put adverse effects as absolute number (i.e. 1.6%): but in reality, 25% could mean 1/1000 while 1.6% always means 1.6/100. But yes, NNT is better yet. Thank you, I agree with what you wrote.
Is everyone on top of their Homocysteine Levels….which the culprit could be from reading the Heart Revolution…..as I said my MD is on top of this.
I have had elevated levels and with a homo formula I’m taking now into my 2nd year my levels are coming down….. Look at this if you have not.
My integrative MD has been doing EXTENSIVE lipid tests the last couple yrs and all my numbers are improved over last year…..and Omega 3’s are a main reason….my triglycrides are 100, last year 139….HDL-C 76, last year 70.
Total chol at 239, last year 237. Homocysteine down, fibrinogen down…
All this is very confusing….labs are giving different results too. She changed labs….can drive one nuts all this. I’m 76 and can’t exercise as I did all my life due to a mess of OA and a mess hip replacement.
I am a 48year indian married woman standing at 5’4″ and weighing 90kg.I have been diagnosed with right ventricular conduction delay.I was not able to complete the stress test not more than a minute. I collapsed on the treadmill.the pulmonary function test resulted obstructive. echo results show TR 2+, concentric LVH. Total cholesterol level is 277mg/dL. Ldl cholesterol is 220mg/dL. Thickened aortic valve of 3.1 collect atrium 2.0 cms.
I have been prescribed with
1. Colopilet 75mg 0-1-0
2.tonact 40mg 0-0-1
3. Nikoran 5mg 1-0-1
4.ranozex 50 mg 1-0-1
5.losartan 25mg 1-0-0
6.deriphyllin retard 150 1-0-1.
My mother passed away due to thrombosis.
Since two days I am having severe pain in my left centre below the ribs,with loss of consciousness and breathlessness.
Would like to know is this life threatening?
My previous reply went to the wrong place, I’m sorry. Yes, I fully agree that you need immediate attention to find out what’s going on. Passing out all by itself is reason for emergency treatment.
go to ER or call doctor asap
I am using “reply”, but not sure it’s working right. I understand what you’re saying, and I do like NNT. But I still feel that we should all avoid EVER using relative numbers in the way the 25% was used. It’s Big Pharma’s way of selling drugs: put the upside in a relative number (25% yay!) and put adverse effects as absolute number (i.e. 1.6%): but in reality, 25% could mean 1/1000 while 1.6% always means 1.6/100. But yes, NNT is better yet. Thank you, I agree with what you wrote.
Hello, My numbers were terrible for a young (er) healthy athletic woman.
Dr. says genetics and wants me on the pharmaceuticals.
I tackled it with an all natural drug called Lipid Shield. So the total number dropped 40 some points and everything was great in every category. (could supply this if anyone is interested, baseline to current ~)
Went off it this summer, just got results, NOT so good. Almost back to where I started.
I am going back on this product. The website looks corny, and it is a proprietary blend, and who knows if there is ligament data… but it works… and is natural with ZERO side effects, was on it for years….made from plants and Red Bean rice extracts, I believe. Dr. said what ever you are doing, keep it up.
Maybe someone with some expertise could research this product and tell my why it works like crazy.
I will tell you one thing if it ever goes public, I am there!
Thanks I may try.
D. Garoni–red rice yeast contains a statin drug (is it lovostatin, I believe?). But the dosages is unknown and could vary. A friend mine used it for a while, got a different batch (probably more potent) and collapsed with muscle/joint/tendon problems. Most statin damage seems not to be permanent, but some definitely is permanent damage.
Red Yeast Rice made me VERY VERY Sick. I couldn’t move. It was so horrible. Lovistatin also did that. I had terrible muscle aches and spasms. Was was put on Zocor, which did lower the LDL, but then I turned up with prediabetes. My mom was on all that stuff and SHE STILL had a heart attack. My dad never had high cholesterol and he had heart disease too. I think the doctors greatly underplay the side effects of statins.
BTW I also know someone that was on Lipitor. He’s a family member and had to stop Lipitor because it jacked up his liver. BTW his liver has not returned to normal and it’s been 2 years. The enzymes are still off all the time.
Yes, although this information is suppressed, it’s certain that statins can cause permanent damage. You can look at websites such as SOS (Stopped Our Statins) or Spacedoc (a former flight surgeon/astronaut with permanent damage). Johns Hopkins Myositis center treats statin-caused autoimmune diseases. These diseases can be devastating, and because they aren’t reported to the FDA by the prescribing doctors, we don’t know how common they are.
Lucy How do I reply to your email?
BTW I also know someone that was on Lipitor. He’s a family member and had to stop Lipitor because it jacked up his liver. BTW his liver has not returned to normal and it’s been 2 years. The enzymes are still off all the time.
Red Yeast Rice made me VERY VERY Sick. I couldn’t move. It was so horrible. Lovistatin also did that. I had terrible muscle aches and spasms. Was was put on Zocor, which did lower the LDL, but then I turned up with prediabetes. My mom was on all that stuff and SHE STILL had a heart attack. My dad never had high cholesterol and he had heart disease too. I think the doctors greatly underplay the side effects of statins.
Reply: Underplay the side effects (adverse effects) and overplay the upside. At best my Zocor prescription would have lowered my cardiovascular disease risk by 2% or so over the next 10 years (from 10% to 8%). Of course I’d be 80 then. (What it did instead is stop my 50 mile hiking regimen and gave me a permanent neuromuscular disease.)
I don’t know how to reply I just pushed box.
LUcy I’m pushing the REPLY box on the email I received. The comments go oldest to newest, and I don’t know how to get to the newest comments. thanks!
Just click “Newer Comments” or “Older Comments” bottom right. Then you can flip pages.
So how do you increase LDL-P without lower cholesterol. I have seen posts suggesting red yeast rice which I understand is just a natural statin that depletes cholesterol and niacin which does same?
Thank you, doctor. I kind of get it, but sometimes there are a dozen pages to try to get through…..
@ howfussiner
I know, it’s quite a lot to get through. There’s a technical reason though. If all the comments are on one page, that particular page will become very slow.
I do understand, but would it perhaps be possible to have the newest come up first? Also, as things stand, one thinks that pushing “reply” to a new post will actually reply to that post, rather than to the very newest one.
I have to second that. It’s extremely inconvenient to have to hit next so many times. Not only that, in Firefox, every time you hit Next, the page scrolls to the top, so you need to scroll down every time. In most places, there are either options for “Newest first”/”Oldest first” and/or pages with the ability to go to last page immediately or any other page. Also, as howfussiner says, “reply” should immediately bring to the post one replies to. Who designed this pages? If there are no options for the blog author to do it, can a defect/design change request be submitted to the developers?
The reply button indeed brings you to the post you are replying to. Just look a bit further down the page and you’ll find the box to fill in your reply.
However threaded comments can only be three levels deep. Therefore it’s best if everybody replies to the original comment.
Let’s say person A writes a comment. Then person B replies. If person C has a say as well it’s best to reply to person A’s comment. If he replies to B’s comment the level will get deeper and the reply button will disappear.
I know the comment system isn’t perfect but you’ll have to take into account that this is not meant to be a chat forum. Comments are supposed to deal with the content of the original blog article itself.
I agree, but on the other hand, I really don’t want to look a gift horse in the mouth. Overall the site is a generous gift and does a lot of good.
I read each of these posts in my email. So I don’t have any of the problems reading the site. I have no idea what they’re talking about.
Thank you Doc. It’s working well here on my iphone here in Nashville, Tennessee. I look forward to your posts!
Responding to where replies appear: I’ll now check to see where this reply appears. It was in response to your “The reply button indeed brings you to the post you are replying to. Just look a bit further down the page and you’ll find the box to fill in your reply.” I simply pushed the response button in my email.
Doctor, again thank you for this site. Sorry to bother you with procedural stuff.
i belong to a website that discusses heart disease in depth. Although it specifically deals with the ApoE4 genotype, many N=1 experiments are conducted.
There are many on statins and many that try solely diet interventions. There are those that tried one statin, had adverse effects, recognized it and tried another with success and no adverse effects.
Many, many deep dives into LDL-P with folks lab results posted. https://www.apoe4.info
Just another source of info if you’re tired of the continual ramblings that have unfortunately dominated here.
This interests me. Are you able to generalize/summarize in terms of what practical directions it’s sent you in? Also, is the SLCO1B1 gene at all mentioned?
Does Bergamot/Bergamont increase the size of lipids or particle count in a beneficial way?
I don’t think my LDL-P has ever been measured, but my latest Lipid Panel results from December 2014 showed my HDL to be 45, LDL 57, Triglycerides 75 and Total Cholesterol 117. I’m not a doctor, but these seem like pretty good numbers to me! I have calculated the various ratios too and all are in the ideal range.
I am a 45 year old male, active, eat a vegan, mostly wholefood diet and my BMI is around 22/23. A few years ago I started to eat more junk food and gained a lot of weight – my BMI was over 30 at my most heavy and my HDL was below 40 and my triglycerides were high. For the past 3 years I have been back the kind of weight I was in my late teens and early twenties and I am absolutely convinced this is the natural kind of weight for me, as my cholesterol numbers went back to normal.
I guess I am living proof (or at least evidence) that lifestyle changes can correct cholesterol problems and drugs are not necessarily the answer.
Andy – just because the lifestyle changes worked for you doesn’t mean they work for everyone. You were fat, your numbers were bad as the result. You lost weight, they went down. There are many of us who are thin – my BMI was 24.3 a couple of months ago when my cholesterol was last measured and my LDL was high (triglycerides low, HDL – 59). Now when your BMI is 30, you drop it to 22/23, it’s a huge difference. Now, I did drop weight in the last couple of months, so now my BMI is 123. I am not yet certain about the effect on my cholesterol – I increased exercise from essentially only walking on weekends to an hour every day and did tinker my diet a little (as I’ve never eaten junk food, I didn’t have much room there beyond simple fewer calories), but I am not certain yet how it’ll affect my cholesterol. 24.3 to 23 isn’t a huge difference – I lost about 8 pounds from 133 to 125.5, my goal is 121-122 (mostly really because of vanity at this point – I want to fit into some skirts I wore a few years back), and given that I am not overweight and don’t eat junk food there isn’t really much changes I can make. For many of us, it’s genetic. I am not planning to take drugs now – with normal bp, normal sugar (without medications), the absolute risk reduction seems lower to me than the risk of side effects, plus, my ratios are all fine, but I am just saying that lifestyle changes may work wonders if you are obese or very overweight and eat junk food, but not always. Genes play a large role too.
Kitty – I would never say that worked for me will work for everyone, but my guess is that a lot of people who are overweight, not exercising and eating badly probably could get their numbers in shape with lifestyle changes. I remember all the times my doctor tried to get me on medication, but I refused as I knew I needed to make changes first.
Of course, people with genetic factors in the mix are going to find it harder and may need the extra help that drugs can give, but I am convinced the number of such people is far lower than those who are actually on these drugs.
Good luck in shedding those last pounds and getting back into those skirts. I have a t-shirt from a concert I attended in my late teens and I can fit in it again now – please don’t hate me too much 🙂
Andy, I’d never go to my college sizes much less late teens. I weighted around 110 pounds back then. I am 5′ 2″ by the way. I don’t even think really it makes sense for me at 55 to do it, my face will look terrible. The thing with women and menopause is that our metabolism slows so much, the fat gets redistributed mostly to stomach, and we can eat 1400 calories and still gain weight. If I don’t exercise, I’d need probably only 1200-1300 calories.
There actually are many people who have high cholesterol because of genes.
Wow, 117 cholesterol…that to me sounds like almost an empty tank of cholesterol.
We NEED cholesterol. And our bodies NEED good fats…
My HDL is 76, LDL 142 (working to get lower), Triglycerides 100 and total chol is now 237.
Some one was saying they take Non GMO lethicin daily to keep arteries from clogging.
All this talk about LDLs–means what? In my case, if I leave my LDLs at 190, my heart disease risk is 10-12%. If I take a statin and slam my LDLs to 100, my risk drops about 2%…over 10 years. Almost insignificant.
Since my triglyceride/HDL ratio is .7, the likelihood is that my LDLs are predominantly of the benign type, rather than small dense BB like. So my risk probably drops much less than 2%.
Perhaps this is why the new and improved “expert” panel guideline to qualify for a statin is 190. This is the AAC/AHA panel in US.
PS. The adverse effect rate on statins is about 10% and can be devastating. I’d suggest much less irrational fear about LDL level, all by itself, and much greater fear about 40% or more of people over 45 on a very strong drug.
These 190 guidelines bug me too because they don’t take the risk into the consideration at all. My 10-year risk is under 2%. The risk reduction with drugs – which I have no intention of taking – would be barely seen under the microscope.
OH Thanks that helps so much. I have the same thing. IT was very weird when they came out with the guidelines they said they made up the 100 number. Now they just want everyone over 65 on the drugs. I think it’s because more than 1/2 the people that get heart disease don’t have high ldl, so they don’t know who should take it. I am still not sure the drug company has come clean on all the side effects either.
SEe they made the LDL target up. https://www.nytimes.com/2013/11/13/health/new-guidelines-redefine-use-of-statins.html?pagewanted=all&_r=0 I think they think that everyone with 190 LDL has familial hypercholesterolemia. I don’t have that. My cholesterol used to be normal when I was younger, and it went up with age. I eat a very good diet. Plus I am not sure they have even studied people with extreme cholesterol. Remember that group of people in Italy, they had cholesterol LDL that was like 2,000 and they had low HDL and 1,000 triglycerides and nobody died of heart disease. I think they need to study people with extreme cholesterol. I know one person with that extreme cholesterol and she has no plaque at all. I know someone else with it that has been on statin for years, and statin does not really work very well on him.
It’s about money and corruption.
WEll I think the rank and file doctor cares. They just believe everything they hear. The drug companies fudged the data on anti depressants. They were not really very effective. They exaggerated their effectiveness and downplayed the side effects. They probably do it all the time. I hope somebody hacks their system and gets the reports to see all the trials. They only need two trials to say something is effective. https://healthland.time.com/2012/09/24/a-doctors-dilemma-when-crucial-new-drug-data-is-hidden/
I agree regarding doctors, but especially when prescribing a drug to someone to prevent a disease that they don’t have…being informed and “doing no harm” are totally connected. The whole preoccupation with LDLs is driven by Big Pharma. Big bad news.
16% of doctors in a recent study acknowledged that they are influenced by pharma reps in their offices; but the same doctors thought that 60% of their colleagues were influenced.
I am with you all believe me on the pharma industry, and on the depression business, yes business, I was suckered in for about 10 yrs when I could NOT get my thyroid supported with those so called labs….once on Armour the depression lifted…then again some yrs later found how deficient I was in Vit D…..that’s a horrible injustice to SO MANY….the Vit D non business.
my elderly mom’s doctor told me she still thinks eggs are bad.(she doesn’t care what the studies say, you know that pesky science thing) The doctor is on a vegan diet and she talks about it all the time. The vegan diet makes her very bad tempered and she gets more arthritic every time I see her. She thinks Statins are God’s gift to the world. BTW my mom’s in an Alzheimer’s unit. Not sure if it’s the drugs, but I don’t think the highest does of Lipitor is good for an 89 year old lady. Her body would probably disintegrate if they took away the Statins. She’s been on that stuff for nigh on 30 years. (didn’t stop 1 her from having a bypass, stents and an eye stroke) I am really not sure, if they help at all, but her doctor swears she would have died without Statins.
I’m sorry to hear of your mother’s suffering. Many of us have statin-worshipping doctors. Few of these doctors base their faith in anything scientific. My first investigation in the US is to check Dollars for Doctors and other sources to find out how much money the doctor and/or the group received from Pharmaceutical Companies.
My second investigation is to find out if the doctors deny the adverse effects that statins cause in over 10% of patients. Last week I met someone (medical technician) whose close friend died of rhabdomyolysis–because the doctor denied that his foot cramps were caused by his new regimen of statins, so he kept right on taking them as ordered. The doctor was, I’m sure, simply ignorant and focused on compliance.
Thirdly, I’d get the doctor’s best opinion on the benefit of statins and the source of his knowledge. One may totally “qualify” for a statin by being in the category of 1% decrease in heart disease risk over 10 years. Now that number makes it simply not worth the risks.
HEre’s something weird. They put me on the Statins. I have had life long high cholesterol but at middle age it went way up. I could barely walk after a week. I switched to another and then started having muscle cramps. I kept it up until I started having higher blood sugars. Then I found out, they might not even help women without heart disease. I tried red yeast rice, which also made me achy and sick. I also tried this supplement called Sytrinol, and that’s where it gets weird. It made my cholesterol go up 30 points. Guess what, I was having the muscle and foot cramps with that too. hmmmm Now that is weird. Stopped the supplement and the foot cramps and muscle aches stop. huh. Right now I am avoiding weird oils (soy, corn, canola) and sugars. (I never was a sugar eater anyway). I started eating meat, eggs and normal dairy. I am sure my cholesterol sucks, but I FEEL SO MUCH BETTER! All the cracked skin is gone. huh weird. You do know that arteries get damaged. Maybe the cracks inside heal too. Well I hope so. Krill oil is good for skin too. Maybe good for arteries inside too.
And then there is the potential downside of statins for example: https://plus.google.com/102631385922452069974/posts/EAu1sWEBjyX
What is “high” cholesterol? Don’t buy into this language and the puerile simplification of this pseudoscience. This is “science” bought by money, not objective research.
Good diet and exercise are of course important. If your LDLs don’t go down, then question what would be the risk/benefit of lowering LDLs with a drug. Maybe you’re already as healthy as can be.
Look at the numbers, like Framingham, etc.–then remember that these studies emphasize benefit only. You will almost certainly be surprised at how small the benefits are…if you express them in objective terms, such as NNT.
The risks? Want to know more?
Again and again and again. You mention muscle cramps. 99% of prescribing doctors never give a warning about cramps…and what continuing with the statin drug might entail.
We’re talking business here, not science. You know–faulty airbags, ignition switches that fail, etc.
I sent Lucy a message and don’t know if it went thru. Some folks on another health board take CholestOff a supp and you can find a lot of reviews on Amazon, could cause some constipation BUT for me I take higher dosing of magnesium daily anyway……
Also one person reported she takes Sunflower Lecithin, not soy lecithin and she believes it helps keep arteries unclogged…I’m probably going to take the Sunflower L as I’d like my LDL to be a little lower….
The “bad”:
LDL-P: 2626
LDL-C: 269
Total: 355
HDL-P: 28.4
Small LDL-P: 630
The “good”:
HDL-C: 70
Trigs: 79
LDL Size: 21.6
LP-IR Score: <25
All 14 values on a comprehensive metabolic panel are within reference ranges.
20 y/o. Works out 3x/week, high intensity, heavy weight lifting. Eats a low carbohydrate, very high fat diet. ~40% calories sat. fat. Regularly consumes olive oil and olives, avocados, nuts, and fish (salmon, sardines). Total carbs hardly ever go over 60 (15-30 g fiber/day). Eats 8-12 servings non-starchy vegetables/day. Sleeps 7-8 hours/night fairly consistently. No smoking, no alcohol.
For someone like me, those values seem weird. On the outside, I am very fit. I'm muscular and lean. And I have plenty of energy.
Perhaps is it because I intermittent fast a lot? Or is it that with the amount of fat I'm eating I also eat too many vegetables/carbs? Thyroid? FH? That I fasted ~18 hours before I had my blood drawn?
Should I be concerned?
Okay this is just my humble opinion. I looked at the studies, and I think the whole cholesterol thing is meaningless. AT best cholesterol is a secondary relationship to heart disease. Before the age of 50 there seems to be a relationship, but after 50 the relationship breaks down. In fact, I think the doctors are wasting their time and money on all this cholesterol lowering. I think the researchers know it but it’s too embarrassing for them to tell everyone that they screwed up. The only drugs that seem to work (although they have terrible side effects) are the Statins. Other drugs and supplements that lower cholesterol have no effect or make people worse. I think that the statins are actually stablizing the plaque and have little to do with cholesterol. IMO just eat regular, non processed food, get off the low fat diet, because it’s never been shown to help anyway. Avoid sugar, avoid stress, avoid vegetable oils and food made in laboratories like artificial spreads. Exercise and get good sleep. Statins don’t help prevent heart attacks in those that never had one. Read the studies for yourself and see if what I am saying is true.
That’s clever thinking Lucy. I think you’re spot on. Study the literature on your own terms and use common sense 🙂
I just got my lab work rushed to me and a letter stating I should take immediate action. Scary!
I’m 59 y.o. white female 5’8 165 lbs.
My total cholesterol is 303
HDL 61, LDL 213, TRI 146
I’ve made many dietary changes over the last 2 years:
Gone from whole milk to fat free, given up sodas, given up chips, given up ice cream, given up my flavored coffee creamer, and eat only dark 70% or higher dark chocolate. I’ve been 90% compliant with these changes and my numbers are worse than ever. I am really afraid of statins. My arteries have only shown mild plaque. Is drugs my only recourse? I am a heavy coffee drinker (1 use 1 Tsp sugar to 16 oz), should I switch to tea? I’d appreciate suggestions
You write: “I am really afraid of statins.” There is very good reason. https://alaswell65.blogspot.com/2015/01/statin-myopathy.html
The risk/benefit is very difficult to gauge, since adverse effects are very rarely reported.
–In my case, in contrast to what my doctor said, the benefit was less than 2% if I took statin for TEN years.
There are fairly consistent signs of upcoming disaster if one is destined for some bad statin effects. Want to know what they are? reginaofthesun@yahoo.com
I am 51 years old, had for the last couple years a blood pressure of 140/95. My cholesterol readings are as follows:
T. Cholesterol:260 mg/dl
Triglycerides:94 mg/dl
HDL:50 mg/dl
LDL:191.2 mg/dl
The doctor prescribed a blood pressure lowering medicine and put me on statin therapy due to high LDL. However, taking statins a couple of times made me feel terrible and I stopped taking the pills and started a low carb, low fat diet with regular exercise since I was eating chocolates and desserts heavily. My doctor says that this will not help much and that I have to stick to statin pills to lower the high LDL, but I do not want to take it because of its side effects.I have read about the NMR test, but we do not have it in Egypt.Can you give me your advice please.
I could be all wrong. The studies I looked at say that cholesterol has very little to do with heart disease. My mom had high cholesterol and heart disease, my dad had low cholesterol and heart disease. 75 percent of people don’t have high cholesterol but they have heart disease. The level of LDL was not related to the level of plaque at all. Cholesterol seems to be weakly correlated with heart disease before 50 but not after 50. Sugar seems to cause heart disease. Too many carbohydrates are not good. Saturated fat has never been shown to cause heart disease, and neither has foods that contain cholesterol. https://www.medicalnewstoday.com/articles/267834.php The doctors like to give people pills, but heart disease is a multi factorial disease. I am trying to reduce my stress level, and eliminate processed foods, sugars, and too many carbo hydrates. exercise… all of these things that doctors do not like to tell people to do because it’s hard and doesn’t involve a prescription. I wish doctors would all stop measuring cholesterol because it causes anxiety and doesn’t really mean that much. The statins don’t really prevent heart attacks but they seem to help, at least a little, once someone has had a heart attack. In other words, there are no easy answers like a pill for heart disease, and people should forget about it.
Thanks, for your comments. I’m inclined to believe as you do, although they’re is a need for certain medications at times, I’m not convinced that this is one of those times. I’m capable of committing to more lifestyle changes; more exercise, losing weight, more fiber, less sugar, less sat. Fats, less animal meat, more fish, and add in a couple heart healthy supplements.
We moved my mom’s kidney % from 15% function to 23% in a year with a very low sodium diet with 98% compliance (she gets to cheat w/small portions on holidays or b.d.); so lifestyle changes when compliant CAN yield results, I’m just hoping it’s enough to push my total and my LDL down.
Do some research on Coconut Oil and Cholesterol issues…..I use CO for everything and why not pick up a book talking about the Cholesterol Myth…..cholesterol is BIG BUSINESS……
My opinion and I’m sticking to it. Check out Weston A Price Foundation and their work on cholesterol and oils in general. We need good fats and Alz is linked to low fat crap…I’ve never bought into the LOW FAT designer foods….I call them. I don’t overdoe and sit down and eat lbs of fat and eat in moderation, but really have cut out carbs a LOT and sugars for sure…these are the killers…..as I see it all. J
I also slashed carbs to less than 5% (low cal, fiberous veggies like broccoli only). High coconut oil, lard, butter, fatty cuts of meat, cheese, cream., yolks etc. My LDL went from 185 to 305 – ouch. I looked into the low carb thing again and found that some low carb guys do recommend up to 20% starchy carbs and claim that many low carb people felt better after adding some carbs. But there are still some hard core guys like Ron Rosedale who insist that there are no safe starches. I need to find out if my 305 LDL is killing me or protecting me (I did go those two years without a cold after years of spending all winter coughing up phlegm)
Joe, it’s great to hear you and other folks questioning the ancient dogma. I honestly don’t know if your present LDL levels should be of concern. As I understand it though, what’s probably most important is the kind of LDL–“good” LDL may exist, as you say.
Here’s what I do know, however, without departing from the mainstream dogma. If I lowered my LDL from 190 to 100, my risk of heart disease would decline insignificantly. My odds of heart disease over the next 10 years, taking me to 80, would go from about 10% to 8%.
Believe me, given the adverse effects, not worth it!!!!
Just google “statin myopathy” to get an inkling.
where did you get the 10 to 8% figure?
Here’s the Japanese study that says that women’s cholesterol rises at menopause but doesn’t seem to be related to heart disease. They recommend diet, but as I said, I have tried for years and have been unable to do anything reduce the LDL with diet. I did the statins for a while, but started to develop prediabetes. (I think the statins cause diabetes) Statins have not been shown to prevent heart disease. That was true for my mom and my dad, they were both on statins and still had cardiac events. I wish they would get all the cholesterol crazy train and try and figure out what really is the cause of the damage to the artery, but well I guess I am dreaming. I think if they got off the cholesterol pony, they could have solved this a long time ago. https://phys.org/news203844242.html
my cholesterol including LDL is drastically affected by diet. I have gone on starvation diets excessive exercise and had cholesterol of 145. LDL 50, HDL 85. I have been on a high high fat very low carb and my total cholesterol 22400 and my LDL 305. if I eat my normal diet about one third fat, one-third carbohydrate, and one-third protein, my cholesterol ends up about 185, LDL 105 and HDL 70
I read the article on that study that you posted. Like most studies a comment on LDL below or above a fairly low number like 100 or 160. But they don’t comment on very high numbers like 300 or 400.
sorry about the above typo, my total cholesterol on high fat is 400 not 22400.
400 total cholesterol
weird…Mine stays the same no matter what! I did not try the starvation thing. Look, at this huh maybe this is why. I have naturally low triglycerides always around 50 to 60. The cholesterol equation has two unknowns. (I was a math major and that is a major no no) Look cholesterol LDL may not be accurately estimated for people with low triglycerides under 100 or over 400. I did notice, if I eat a LOT of sugar, which I don’t usually do, my triglycerides go up a little.
I don’t know if I posted link. See, I think it might depend on person. My cholesterol does nothing at all no matter what I do. (Haven’t tried starvation) https://www.ncbi.nlm.nih.gov/pubmed/18426324
Lucy
Low triglycerides and high HDLs correlate with low percentage of your LDLs being bad, and more of your LDLs being “large fluffy” good.
Having had it happen to me, with similar lipid profile, I’d warn you strongly that statins can cause horrific diseases in some people. Other people (I saw one yesterday at the health club) don’t “recover” for months and years–and may only “recover” because they eventually attribute aches and weakness to age.
Lucy–As you know, the “cholesterol pony” as you call it has not much to do with our health. By the standards like Framington’s, my own risk of CVD was lowered by less than 2% over the next 10 years. Insignificant. (Lowered from 10% to 8%: I can’t get it lower, even by getting my LDLs from 190 to 100–because my age alone keeps me at 8%).
Note: You will hear my situation described at “lowered heart disease risk by 20%”, and even many doctors are naive enough to get sucked into this trickery.
For example, lowering someone from .01% down to .008% is a 20% reduction.
If we raised the time period from 10 years to 10 million, I’m sure that the resultant lowering would get larger.
This is true deceptive and unscrupulous drug-pushing. I wish our doctors could/would save us! Just do no harm–don’t write the prescriptions!
If this question about 8-10% is directed to me, I simply went to the standard “heart risk evaluators” on the Internet –like Framington–and entered my data. If people want, I can give more details.
I know. I have family members that were hurt by STatins with permanently damaged livers. I took them for a while, but could not stand it. As I said, that LDL number is not even accurate for people with low triglycerides or extremly high triglycerides because the equation doesn’t work for them. Triglycerides go down when sugar and carb consumption go down. Low triglycerides RAISE LDL even when accurately measured. They do by their very nature, because the residual of the triglycerides is LDL which is then recycled by HDL! High carbs and sugars raise triglycerides(lower LDL) and causes more DIABETES riskTOO!
I am sure no doctor would suggest eating lots of sugar to reduce LDL. (that also reduces HDL) Saturated fat raises LDL and HDL a little, but it’s not significant. I think they all need to stop with the cholesterol and focus on the triglycerides. THat number needs to go down and also the blood sugars need to be kept down or they are going to give poeple heart disease and diabetes. If they keep focusing on the LDL they are going to make people diabetic and that’s exactly what the statins do, they turn people into diabetics. THe low fat diet had very little effect on my cholesterol. I don’t eat sugar and never have, and that’s probably why my lipid profile looks like that.
Lucy–I had those kind of blood lipid levels too. Exercised 8-10 hours a week intensely (training for adventure travel), ate no refined sugars or carbohydrates, felt great. But now I’m “cured”. All I needed was a statin drug, pushed and pushed and pushed on me by doctors, in order to be cured of my “LDL” disease. The “side effect” of this cure is that I can’t walk more than 10 minutes now, can only exercise about 3 hours a week, am in constant pain and fatigue.
Six months of a statin changed my life forever. Statins may (or may not) have prevented something that never happened. But for sure they caused things that never ever should have happened.
Money.
There’s a website where you can report Statin side effects. I took them for a while and had intense muscle pain. I switched to another which worked for a while, but then caused muscle cramps. Then I started to turn up “pre” diabetic. No family history of diabetes, normal weight… I got off easy compared to my brother and you. I am hoping I can make my blood sugars go down. They used to be fasting 85 but now they are a little over 100. A1c kept going up from 5.3 to 5.7. The doctor’s answer was take another pill for that.
“Dr Collins, who championed the controversial drug, said the additional work was needed to convince the public that statins were safe.” That sure doesn’t sound like the beginning of an objective study, does it? (Rory Collins is a major statin drug pusher–big dollars from Big Pharm. Huge dollars.)
Lucy, what’s the site to report statin damage? Thanks!
https://www.statineffects.com/info/ I heard some doctors at Harvard got in trouble for saying something about drug companies over stating benefits and understating side effects of STatins.
Hello. I have been reading your blog and wanted to get your thoughts on my profile. After reading about this topic I asked my dr for these tests. When the LDL-P came back so high he suggested I see a lipid specialist, however there are none in my area. A cardiologist said I should take statins which I do not want to do. I am considering having some tests for inflammation done to add to the picture. Would appreciate your thoughts. I am 60 yrs, 5’5″ and 168 lbs. I have been working on diet by increasing protein and lowering carbs and am down from 173#. I have not smoked in 30 years. My mother and brother died of heart disease, my father had a heart attack but died of brain cancer.
LDL-P 2055
LDL-C 141 0-100 mg/dL
HDL-C 64 40-200 mg/dL
Triglycerides 134 0-150 mg/dL
Total Cholesterol 232 0-199 mg/dL
HDL-P (Total) 40.9 30.5-100.0 umol/L
Small LDL-P 851 0-527 nmoles/L
LDL Size 21.4 20.5-100.0 nmoles/L
Large VLDL-P 2.5 Comment: Graphical report available upon request. nmoles/L
Small LDL-P 851 Comment: Graphical report available upon request. nmoles/L
Large HDL-P 7.3 Comment: Graphical report available upon request. umol/L
VLDL Size 42.4 Comment: Graphical report available upon request. nm
LDL Size 21.4 Comment: Graphical report available upon request. nm
HDL Size 8.9 Comment: Graphical report available upon request. nm
LP-IR Score** 34 Comment: Graphical report available upon request. 0-100
Glucose 107 70-99 mg/dL
Hemoglobin A1C 5.3
Glycohemoglobin 6.1
Deborah
I agree that lowering LDL-P may be important in your case. There are some signs of insulin resistance with a BMI of 28, relatively high TG and elevated glucose (assuming it was a fasting blood sample).
I’m usually a bit reluctant with statins in cases like yours. Your LDL-C is not that high really and statins may increase the risk of diabetes.
I believe you should continue avoiding sugars and restricting carbs. If you do that, increasing healthy natural fats is fine.
But, of course you should follow your doctor’s advise. He/she knows you better than I do. He/she is probably worried about your family history and feels that statins may help reduce your risk which may very well be right.
My opinion is only a general view on the issue.
Thank you for your fast response. My fasting blood sugar is on the high side, but oddly my LP-IR score is low. I am going to be re-tested soon. I am hoping that increased exercise and diet changes will have an impact. I worry about CVD, but don’t want to trade for Diabetes. What additional tests would you recommend? From what I have read, the real culprit is inflammation.
What is the definition in this context of “inflammation”?
What test or test(s) are there to measure inflammation?
Thank you. David
You’re right.
The low LP-IR score doesn’t suggest that insulin resistance is a big problem yet.
TG/HDL ratio is not that bad either, thanks to your relatively high HDL-C.
I would probably not recommend any further testing at this moment.
Focus on the lifestyle issues, healthy diet and exercise.
But again. Listen to your doctor.
Good luck.
hs-CRP is the most commonly used test to detect chronic low grade inflammation
https://www.docsopinion.com/health-and-nutrition/hscrp/
https://www.docsopinion.com/2013/05/03/inflammation-and-heart-disease/
hs-CRP is the most commonly used test to detect chronic low grade inflammation
https://www.docsopinion.com/health-and-nutrition/hscrp/
https://www.docsopinion.com/2013/05/03/inflammation-and-heart-disease/
hs-CRP is the most commonly used test to detect chronic low grade inflammation
https://www.docsopinion.com/health-and-nutrition/hscrp/
https://www.docsopinion.com/2013/05/03/inflammation-and-heart-disease/
Dr Sigurdsson,
May I please have your thoughts regarding the niacin experiment I conducted on myself. When my LDL-P shot up from 366 to 1320, I increased my Slo Niacin from 500 mg to 1500 mg. Now, 3 months later, my LDL-P has dropped to 972.
FYI, I initially posted at length 3 months ago.
Thank you.
Niacin is known to lower LDL-P. The effect may vary somewhat between individuals. Drugs that lower LDL-C usually lower LDL-P as well as discussed in the blog article above.
Sorry I wasn’t able to respond to your initial comment.
Thanks for sharing your thoughts.
Although niacin appears to work well for me, I’m alarmed by the HPS2-THRIVE findings of its worrisome adverse effects and risk-benefit profile.
However, it is my understanding that the AIM – HIGH study tested niacin as an additive to statin therapy. And the HPS- THRIVE study included laropiprant which may have skewed the results.
So I’m conflicted – I have a family history of heart disease and I’m trying to be proactive.
Thank you again!
Taking niacin it seems prudent not to take carbs in the following 6 hours. I have checked it myself with a glucometer.
The HPS-TRIVE study showed that adding niacin/laropiprant on top of statin therapy was not helpful for people with cardiovascular disease.
Earlier the AIM-HIGH trial had shown similar results.
So, although Niacin positively affects blood lipids, randomized clinical trials have failed to show clinical efficacy of this drug. This is the main reason it’s not widely recommended, although it may raise HDL-C and lower LDL-P as well as Lp(a).
Niacin hasn’t been compared to statins in primary prevntion.
I’m confused. I thought that reducing my LDL-P would improve my coronary risk profile and that I could thus use it as a measurement tool. However, the studies are showing that despite the drop in LDL-P, one’s coronary risk is not improved? So then how would one gauge one’s progress in primary prevention?
Thank you again. I apologize for my confusion!
I know Zooie. These issues are complicated.
LDL-P can be regarded as a “surrogate marker”. We have many examples of such markers. Cholesterol, blood sugar, LDL-cholesterol, hs-CRP, blood pressure etc.
So, although LDL-P is associated with risk, it hasn’t been proved in a clinical trial that lowering it is always beneficial. Of course, clinical efficacy may also depend on the method you use to lower it (diet vs. drugs etc).
For example statins lower LDL-P and they seem to positively affect cardiovascular risk. That doesn’t mean that lowering it by all other measures is helpful.
What we know is that adding niacin to statins doesn’t lower risk, although it lowers LDL-P and raises HDL-C. However, this doesn’t tell us anything about whether niacin will reduce risk in people who don’t take statins.
We don´t know whether niacin lowers risk among healthy people with elevated LDL-P. This question hasn’t been addressed in a randomized clinical trial.
Here’s an overview of clinical trials performed with niacin.
https://www.trialresultscenter.org/TRC_m326.htm
Unfortunately, most of the studies are small (except for AIM-HIGH and HPS-2 Thrive) and in most cases niacin has been tested as an additive to other medications.
In the placebo controlled CPD study from 1975 there was some reduction in coronary events by niacin compared with placebo but no effect on mortality after 5 years. However an eleven year follow-up suggested a positive effect on mortality by niacin.
https://www.medscape.com/viewarticle/750937_4
Unfortunately this hasn’t been confirmed by another trial.
“For example statins lower LDL-P and they seem to positively affect cardiovascular risk. ” Dr Sigurdsson, where does the data come that supports this? (I understand that you write “seem” rather than “do”, but that difference is too easy to miss.)
David. There are a number of studies showing that statins improve outcome, particularly in secondary prevention. The evidence is less clear in primary prevention. If you look around my website you’ll see I’ve discussed this issues in a number of blog posts 🙂
Dr S, thank you. Yes, I never advise secondary prevention folks to drop their statin: I don’t know much about it, and not being an MD, I don’t suppose that I need to. But by far most statins are prescribed for “primary prevention”, which I put in quotes because this phrase is anything but neutral. You say the evidence is less clear, but I question whether there is any evidence at all. In fact, I think we should toss out the phrase “primary prevention” until we have convincing, unbiased evidence that this is the case. Let’s return to “first do no harm” for now, especially since we’re treating people who are actually healthy.
Thanks David
Sounds like your view on the issue is not very far from mine https://www.docsopinion.com/2013/10/19/statins-for-healthy-people-tweaking-the-numbers/
https://www.docsopinion.com/2014/04/07/side-effects-of-statins/
https://www.docsopinion.com/2014/01/07/statins-for-elderly-people-was-the-message-corrupted/
https://www.docsopinion.com/2015/03/15/cholesterol-and-diabetes-time-to-let-the-cat-out-of-the-bag/
Dr S, thank you for the additional information and for your blog – they’re both much appreciated. I’ve learned a great deal from your excellent blog. So it appears that only the 1975 CPD study tested niacin alone and the results were positive. Looking at niacin’s negative side effects , my fasting blood sugar has risen to 105 but I’ve not experienced myopathy (as I had when on vytorin). And the serious side effects identified in the more recent studies appear to be associated with the usage of niacin as an additive to another drug.
In addition to the drop in LDL-P, my small LDL-P also dropped from 188 to 133. Per https://www.ncbi.nlm.nih.gov/pubmed/21981843 “Small LDL-P was a strong, independent predictor of the presence of CAC”.
https://www.medscape.com/viewarticle/447166_4 “The presence of predominantly small LDL in an asymptomatic population reflects a three-fold increased CAD risk that is statistically independent of many cardiovascular risk factors including LDL-C. Identification of this disorder in patients with existing CAD identifies one of the most common metabolic disorders contributing to CAD and identifies a group of CAD patients more likely to show rapid arteriographic progression or new lesion formation if not treated appropriately. …. Change from small-dense to large-buoyant LDL subclass distribution now appears to be one of the most important aspects of CAD management in regard to disease progression or stability and requires therapies that are often the least expensive and include loss of excess body fat, exercise, dietary modification, nicotinic acid, and fibric acid derivatives.”
8 years ago, my coronary heart scan put me in the 93th percentile; a repeat heart scan the following year brought me to the 94th percentile. (FYI, my brother’s heart scan put him in the 98th percentile.) Since my initial heart scan, I’ve cleaned up my lifestyle as much as possible – now eating a low carb diet with minimal meat and processed foods and adding daily exercise.
So my quandary is to decide how best to further minimize my coronary risk, given a strong family history of heart disease. I do now understand that the method used to lower LDL-P may be a key factor, and not only the resulting numbers.. However, the old CPD study tested niacin alone. So I guess it’s a risk-reward decision and I’m attempting to do the best that I can with the available information.
Any further insights would be much appreciated. Thank you again. zooie
We focus on LDL because Big Pharma has drugs that lower LDL: massive business. We don’t have drugs that lower triglycerides, as far as I know. Raising HDL with drugs hasn’t proven effective (lucrative) as far as I know.
David
Gemfibrozil s a drug that has been used to lower triglycerides. However, it has not been shown to improve outcome.
Marine derived omega-3 (fish oil) also lowers triglycerides but you need a certain dose to achieve this effect.
https://www.docsopinion.com/2014/10/16/benefits-of-fish-oil-and-marine-derived-omega-3-fatty-acids/
You’re right about HDL-C. Although low levels are associated with risk, raising it with drugs hasn’t been shown to reduce risk.
I don’t know if my reply went through…..
Doctor, you write: Gemfibrozil s a drug that has been used to lower triglycerides. However, it has not been shown to improve outcome.
In this way Gemibrozil is like statins when used on people who’ve not had CVD: they lower LDL, but aren’t shown to improve outcome.
If there are no adverse effects, I suppose it’s okay, though expensive, to prescribe both substances to everyone. In fact, 25% of Americans over 40 are indeed on statins–and the huge majority have not had CVD.
But of course there are adverse effects. Not shown to improve outcome; not shown to be free of adverse effects; prescribed to millions and millions of people. Doesn’t this, sincerely, seem insane?
“These guidelines are written by experts in the field and their conclusions are derived from evidence from randomized clinical trials.”
Does anyone really trust these “experts”, and if so, why? Half the panel is formed by American Heart Association. This organization has a list of “Heart Check” foods–a very long list, since they get paid for each one. Dozens of foods from Boar’s Head, Sarah Lee, etc. Some of these foods have 400 mg sodium per 2 oz serving.
I recall a long lecture about cutting down on sodium from the cardiologist that pushed simvastatin on me. Bad for my blood pressure he said.
Dr Sigurdsson, there is lots of madness for money going on. The bottom line (and I’m not talking about you) is that the tens of millions of statin prescriptions are written by physicians–who for reasons I simply don’t understand, defer to the “experts”. We all know that the majority of the ACC/AHA panel has ties to Big Pharma. Please, physicians need to be our protection from these “experts”!
“Niacin hasn’t been compared to statins in primary prevntion.”
Why, logically, would anyone want to do this? If statins aren’t demonstrated to improve outcome with primary prevention, why compare anything else to statins?
Talking about statins seems to transcend logic–even with the very best healthcare professionals. The statin sales pitch, though not based on science, has been dumbfoundingly effective.
Clinical guidelines in the US, UK (and most other countries) recommend the use of satins in primary prevention for individuals at high risk.
These guidelines are written by experts in the field and their conclusions are derived from evidence from randomized clinical trials.
So, obviously these experts believe that statins improve outcome, even in primary prevention. If that’s the case, it would be logical to want t know if niacin is better or worse than statins?
Zooie
Niacin is known to lower LDL-P. The effect may vary somewhat between individuals. Drugs that lower LDL-C usually lower LDL-P as well as discussed in the blog article above.
Sorry I wasn’t able to respond to your initial comment.
Thanks for sharing your thoughts.
When we get a list of side effects with a medication, who writes that list of side effects? Thank you. David
Okay this is just my non professional opinion. People are putting WAY too much stock on LDL. Most people don’t even know their blood sugar numbers. My doctor told me that my risk of diabetes didn’t really matter.(blood sugars went up on statins and never had a problem before) That makes no sense to me, none at all. She said, people dont’ die from diabetes but from the complications huh? That makes zero sense. Why are we treating a disease, I don’t have (heart disease), and I might not get. giving me another disease. IMO something bad has happened in medicine.
Lilyrose, I totally agree. We could also look at triglyceride/HDL ratio, which is much more predictive of CVD than LDL is. But we have very lucrative drugs, and more importantly new “blockbusters” in the pipeline that lower LDL. And that’s the science
High triglycerides are caused by eating too much sugars and starches. I guess there’s not much money on getting that out of the diet. IMO that’s the association of high cholesterol and heart disease. The triglycerides and the HDL go together like a horse and carriage.
Lilyrose–You seem as cynical as I regarding the statin/cholesterol sales pitch. I guess you know my story. If I’ve heard and forgotten yours, I apologize. Or maybe, hopefully, you’ve just been doing objective reading.
Does anyone know who is responsible for the lists of side effects that come on the labels of our medications? Who writes them?
Both read and a victim of STatin use. Nothing wrong with me at all but high LDL and statins hurt me and took months to recover.
“Nothing wrong with me at all but high LDL…” We get sucked into the language, no matter that we know better. The selling of statins, which has been a massively lucrative drug, was based on the “high LDL” sales pitch. More than likely, your “high” LDL is no longer “high”: the same “experts” (ACC/AHA statin guideline panel) just raised the LDL number to over 190.
A well-known cardiologist from Cleveland Clinic exclaimed, “They’re just making these numbers up out of the air”
So I’m “cured” of my “high” LDL. But how do I cure myself of this?:
https://plus.google.com/102631385922452069974/posts/EAu1sWEBjyX
my triglycerides were 67 and my hdl was something like 65. My LDL was 210.(total cholesterol was like 280) The thing is it used to be lower but as I inched toward 48 years old the LDL numbers went up. I have even read that LDL is just an estimate, so when triglycerides go below 100 the number of LDL is no longer an accurate estimate. I tried this supplement called Sytrinol which made my cholesterol rise. EVerything makes it rise. The only thing that makes LDL go down is statins. I could drink water and eat carrots and brussel sprouts all day and my LDL would be high. I have been hearing that I am going to die from a heat attack for the last 20 years.. A long time ago, I even tried a vegetarian diet and that only made my cholesterol go down 10 points. I exercise all the time and the LDL just stays like that . If I eat lots of vegetables, which I have been doing, my HDL rises and of course so does total cholesterol and LDL and then I get the “you are going to die lecture” again. (pushing the statins)
My numbers were triglycerides 67 and HDL 88. That was good enough for my EX-cardiologist to prescribe…yes, STATINS! Google “statin myopathy” and find “David Alas” and see the results in just 7 months.
My EX-cardiologist said, “You can’t control it with exercise or diet”. What is the “it”: LDLs, of course.
LDLs are NOT a disease. Check Framington and other heart risk evaluators (the places that statin-pushers themselves send you to) and you’ll be reassured to find that even by their primitive calculations, statins don’t do anything meaningful for what’s called “primary prevention”. In other words, you lower LDL but not CVD in any meaningful way.
Now I can’t walk. I’m in constant pain. But on an arm bicycle, I’ve worked up to 45 minutes at 85-90% max pulse rate. When I stop, my pulse drops 35-40 beats in one minute, down to under 100.
Trivial or no benefit, potential devastation, no reliable data regarding frequency of adverse effects.
I am so sorry. At least your liver still works. My muscle problems went away, but my doctor swears I am going to die of a massive heart attack with LDL this high. Well everyone’s gotta go sometime and at least I’ll be functional when I go. I know someone that might permanent liver damage from Lipitor. Not to make it worse for you. Once triglycerides fall below 100 that LDL number is nolonger accurate. Also if triglycerides are over 200, the number LDL is not accurate. They use an equation to get that number. So your LDL might not have even been abnormal. If I use a different equation (developed by the Iranians) my LDL number falls by 50 points. BTW the whole diet controls LDL is BS sorry, it is. You can’t lower LDL with diet except by microscopic amounts unless you lose weight, but if you are normal weight diet doesn’t do sh*T. You can lower triglycerides which indirectly lower LDL. You know all that crap about oatmeal lowers cholesterol? It’s BS you have to eat like 5 bowls of it. IT’s also crap that fiber is good for you, it will raise your blood sugars. Too much fiber is not good for you, in fact all that fiber stuff is mostly nonsense.
Todays world of all these labs is just NUTS…my folks lived into 90’s and NONE of these labs EVER…and they ate everything and NO WAY exercise nuts…no way….and hardly drank any water….not like today at all. And sadly what water they drank and bathed/showered in was/is FLUORIDATED…..
So are our FOODS so out of control than it was many yrs back….
Or is it MOSTLY all the drug world and finding ailments for all these drugs….
Both: call it the Big Food/Big Pharma Complex. I’m completely serious.
NO ONE KNOWS??????? THIS IS FRIGHTENING!
Does anyone know who is responsible for the lists of side effects that come on the labels of our medications? Who writes them?
I assume that in most countries this is a collaboration between the drug manufacturer and federal drug agencies. Registering a new drug is a complex and tidy process involving a lot of regulations. So, I admit I don’t know the details.
Thank you. I myself assume that all the warnings are written by the drug manufacture, no supervision. In studies like the Jupiter study, stopped “for benefit”, these side effects are only those that are found in the two years of the study.
The adverse effects after than are not required by law to be reported. Does anyone think that they are reported?
And even the first, Big Pharma produced warning list plays statistical games. For example, instead of saying that 10% of people get muscle pain, the companies divide muscle pain into a bunch of different categories. Thus it appears that the odds for any given adverse effect is only 1% or .4%, and who cares about such small risk? But added up, a different (and more honest) assessment.
That’s what I’ve been able to ascertain/assume/extrapolate. But as a physician, Dr Sigurdsson (and a physician I sincerely admire), you’ve said that you don’t know the details. The fact that even the best physicians don’t know who determines and publishes the side effects is very frightening!!!!
All that data that drinking 8 glasses of water is good, is bS. No science behind it at all. Just drink when you are thirsty. All these prevention checks IMO are just stupid. In fact, they lead to over treatment which kills people. I know three young women who had their thyroids removed. THat many people can’t have thyroid cancer. I think they “find a little something” then tell people they have cancer and remove thyroids for nothing. I know a lot of women that had 4 and 5 breast biopsies and were treated were over treated for ductal carcinoma insitu. (they don’t even know if that is cancer) One woman died because they gave her radiation on her lung and caused pulmonary hypertension and she died. I do know some people that were saved that really had cancer, the problem is, is they are over diagnosing people for “prevention”
To Lilyrose: I appreciate your writing: “I am so sorry. At least your liver still works. My muscle problems went away, but my doctor swears I am going to die of a massive heart attack with LDL this high.”
It does help to get a bit of empathy from you, instead of denial that this happened that I receive from so many doctors.
But although my liver seems to still work, there are so many very strange things going on with my body now that I’m not certain what’s working or not.
If your doctors swears that you’re going to die of a heart attack, get rid of that doctor as injurious to your health. I know that my EX-cardiologist and my EX-PCP are bad doctors: I got rid of them, and have been lucky enough to find some outstanding good doctors.
I simply don’t go to doctors who buy into the simple-mindedness of the LDL approach to heart disease. I know that they’re massively over-prescribing statin drugs, based on no science and closed-mindedness to science. They write prescriptions based on “expert guidelines”, but they ignore conflict of interest and even ignore actual data.
These doctors are dangerous and harmful people. I’ve seen healthy people get sick from statins that were prescribed by the same doctors that prescribed to me—long after my own disaster. These doctors (unlike Dr S, for example), are doing more harm than good. I don’t expect every doctor to be knowledgeable about statins: but I disrespect any healthcare professional who prescribes without knowledge–ignoring the dictum “First do no harm.”
I have an insurance that has very limited choices. I looked at pictures of your damage. I hope it gets better. I started having that muscle shrinkage thing, but stopped the meds ASAP. I am so sorry you were not as fortunate. I am hoping it gets better foryou over time. I know one person that had liver damage and it’s been two years. The liver is still not right. I wish someone would blow the lid off this. I do not think the numbers of people getting this is small. I think the majority of people have side effects.
Here’s another thread where your discussion might fit better
https://www.docsopinion.com/2014/04/07/side-effects-of-statins/
Doctor, I understand and respect how the discussion fits better under the topic of statin adverse effects. But at the same time, the risk/reward question is so rarely put into one picture. If we know there are adverse effects, and if we don’t know that statins have any PRIMARY prevention benefits at all, then unless I’m missing something, there is no reason to ever prescribe statins for primary prevention.
Thank you for your kind wishes, and I’m really sorry about your friend. I was only on 20 mg simvastatin for 7 months. The warnings were there–but not the ones on the label or the ones my doctor told me about. My doctor asked me if I’d rather risk slight muscle discomfort or have heart disease. The first sign is cramps, usually in the feet, sometimes also in the calves. When I told him that I wished he’d mentioned this to me, the sea-lawyer response was: “Cramps are muscle discomfort, aren’t they?” I retorted, “Yes, so is getting shot in the leg. Now why are you acting like this, doctor?” There are tons of people who get foot cramps from statins: honest truth, I met four new people last week. About a month ago, a friend of someone I know died of rhabdomyolysis–though he’d been warned about foot cramps, not by his doctor, but someone else. His doctor simply kept him on the statin–not trying to kill him, of course, but killing him out of simple ignorance.
Zooie You had myopathy from an LDL-lowering drug (and HDL raiser, if that’s relevant here) and your STILL buying into the LDL-lowering story? All I can say is DANGER! Google “statin myopathy” and see my blog: the photos are the relevant part. Seven brief months on a statin, have been like this for 3 years: quite painful, and I can’t walk any distance at all. All the men in my family got heart disease around aged 60. In fact, all my family either died before that age of cancer or else got heart disease. BUT lowering my LDLs from 190 to 100 lowers my CVD risk from 10% to 8% over a full TEN year period. In other words, I’d have 8% risk until aged 82. But age alone puts me at 7.5% risk.
Previously I was apparently in great health: trekking for weeks at age 68 in the Himalayan mountains, as just an example. Now I can’t walk. But on an arm bicycle I can “ride” for 45 minutes, running my pulse at 85-90%. I can comfortably run my pulse at 140 for the last ten minutes if I want, and when I stop, my pulse drops to 100 in just one minute.
Why do so many doctors simply ignore all this and still talk about statins to me?
one of my biggest questions having both high LDL and lpa is it is more important to lower LDL or work hard to lower lpa they contradict each other so if i work to lower LDL (high carb, low fat, low animal protein, high plant fat and protein, soy, dark chocolate) or work to lower lpa (No SOY, No CHOCOLATE, low plant protein, and fat, higher saturated and animal and dairy fat, low carb)
ive never gotten an answer so every single day i stress about what to eat.
Hi Amy
OI understand your dilemma.
There is quite much individual variation when it comes to the effects of dietary choices on blood lipids. So, I guess the only thing you can do is try it out for your self.
If you limit saturated fat your LDL-C will probably drop. You can check what effect this has on Lp(a) in your case. However, in general, dietary choices seem to do very little for Lp(a) levels.
The experts still consider LDL-C to be the primary target and Lp(a) as a secondary one.
Who are “the experts”? In the US, the “experts” are a panel made up of ACC/AHA. As the NY Times reported, the majority of the “experts” have financial ties to Big Pharma. Statin drugs are the biggest drug blockbuster of all time: they’ve been pushed to lower LDL.
Who are we taking advice from? Look at the AHA “Heart-Check” food list (AHA gets paid for each food tested). Sarah Lee, Boars Head meats with 400 mg sodium/2 oz serving. Bad folks here!
The LDL statin recommendation was suddenly raised from ideally under 100 to 190 at the last “expert” panel meeting. That would have saved my life. Just look at my “david alas” blog under “statin myopathy”: 600 hits a month. A famous Cleveland Clinic cardiologist, in response to the new guidelines, said, “They’re just making these numbers up out of the air.”
I agree regarding types of LDL: I asked my ex-cardiologist if a great triglyceride/HDL ratio didn’t correlate with low levels of small dense harmful LDL. The arrogant fool said, “The science isn’t there yet.”
I need to learn more about Ipa and welcome all advice.
But I know only too much about LDL. Look at risk evaluators, like Framingham. In my case, lowering my LDLs from 190 to 100 would reduce my heart disease risk by 2% over the next ten years: insignificant.
But my ex-cardiologist pushed a statin drug on me and now I can’t walk. Google “statin myopathy” and on the first page you’ll see this blog https://plus.google.com/102631385922452069974/posts/EAu1sWEBjyX.
The fact that it gets over 600 hits a month says a lot. I meet statin-damaged people all the time.
Here’s an article from my blog on Lp(a) and some accompanying discussion that you may find helpful.
https://www.docsopinion.com/health-and-nutrition/lipids/lipoprotein-a/
Dr Sigurdsson, thank you. If I understand correctly, this is what my ex-cardiologist was referring to by “inflammation”. I should have asked if there was a test for inflammation–if so, I’ve had the apolipoprotein B test: is that similar to the Ipa test? If so, mine is fine. But too late, since I have a permanent statin-triggered neuromuscular disease.
Severe damage from statins is not reported, but it’s infinitely more common than most doctors realize. Poor John at the health club was using the stairs multiple times a day to the 11th floor of his apartment: short-term statin regimen, and now his legs are in constant weakness and pain from the hips down.
I took a pulmonary function test recently, wearing my “STATIN DRUGS KILL” T-shirt. The technician printed a piece of paper and handed it to me. It was the obituary of a friend who’d died of rhabdomyolysis 3 months previously. She said she’d warned him that the cramps that soon followed statins could be dangerous–but his cardiologist said to keep on with the drug.
Rhabdomyolysis following statins is supposed to be one in a million. The only way this can be “true” is by not reporting cases like this.
A question for the Doc:
What about situations where LDL-P is high, but the small LDL-P count is low? Would you focus on particle count or on particle size?
For example, some numbers from a recent LabCorp (US lab company) test:
LDL-C: 139
HDL-C: 48
Triglycerides: 138
Total Cholesterol: 215
LDL-P: 1716 (nmol/L)
HDL-P: 32.0 (umol/L), LabCorp Reference Interval, Should be > 30.5
Small LDL-P: 398 (nmol/L), LabCorp Reference Interval, Should be 20.5
(I’m note sure whether the LDL size refers to most common size, or to the average size.)
Jeffrey
That’s a very relevant question and I don’t think the experts really agree on what would be the best way to answer it.
I do think that size and number both may play a role. In general, small particles seem to be more atherogenic than large particles. However, large particles may be atherogenic as well. For instance, patients with familial hypercholesterolemia (FH) often have predominantly large particles and they certainly are at risk of atherosclerosis.
However, particle number is probably more important than particle size when assessing risk. Usually though, if particle size increases, particle number will probably drop. Small particles carry less cholesterol. Therefore more particles are needed carry a certain amount of cholesterol if the particles are small compared to if they’re large.
Thank you for your reply. I would seem to be an ideal candidate for a lower carb diet, Mediterranean diet.
I think that the following study, excerpted below, is perhaps the most compelling about the TG/HDL Ratio. The study showed that patients in the highest quartile of TG/HDL Ratios, e.g., Tim Russert, were 16 times more likely to have a myocardial infarction than those in the lowest quartile.
Fasting Triglycerides, High-Density Lipoprotein, and Risk of Myocardial Infarction
https://circ.ahajournals.org/content/96/8/2520.full
From what I have read, a TG/HDL Ratio of 3.5 seems to be the dividing line between predominantly Type “A” LDL particles (less than 3.5) and predominantly Type “B” particles (over 3.5), although a study found that children and young adults started experiencing arterial damage over a TG/HDL Ratio of about 2.7. You may recall that the late Tim Russert died, from a massive heart attack, with a wonderful LDL number (67), but a sky high TG/HDL Ratio (9.4).
Incidentally, the NMR particle count values shown above are mine (59 year white old male, with well controlled mild hypertension).
In perusing the Internet in regard to the particle count versus particle size question, I found a fascinating case history, linked below, for a 45 year old female, JM:
https://www.lipid.org/sites/default/files/advancedlipidtest.pdf
Her particle count test was a NMR test, so the test should be comparable to mine.
Cholesterol 250
HDL 56
TG 220
LDL 150
TG/HDL 3.9
LDL-P 2,552
Small LDL-P 1,732
Note that her small LDL-P was 68% of the LDL-P total, and her Small LDL-P count was 330% of the LabCorp reference limit (527), while my Small LDL-P was 76% of the Small LDL-P reference limit.
Also note that her TG/HDL was 3.9, versus my most recent value of 2.9 (up recently from prior values of about 2.2). In other words, she is on the wrong side of a 3.5 TG/HDL Ratio, while I have consistently been on the right side of 3.5, and the Small LDL-P values for both of us are consistent with the TG/HDL Ratio data.
The kicker is the American Heart Associateion Coronary Artery Disease (CAD) Risk Calculator:
https://my.americanheart.org/professional/StatementsGuidelines/PreventionGuidelines/Prevention-Guidelines_UCM_457698_SubHomePage.jsp
It shows JM’s 10 year risk to be 1.00% (one percent), while mine is almost 10%. Of course, gender plays a big role (a woman with my values would be below 5%), but in any case, JM’s Small LDL-P values are more than four times greater than mine, while the risk calculator puts my risk at about 10 times greater than hers.
Delete
I am a 55 yr old male, 5’9 and 178 lbs. Previous smoker, quit 7 yrs ago. I walk 3-4 miles a day at the farm, but don’t lift or exercise at a gym. Today I got the lab results back from the doc and they got my attention. He would like to use Crestor and Zetia. Thoughts?
Blood pressure: 150/102
HDL-C: 41
LDL-C: 141
Triglycerides: 245
total Cholesterol: 228
LDL-P: 2238
HDL-P: 36.4
Small LDL-P:1264
APO A: 125
APO B: 124
Ratio:.99
Hs-CRP: 5.8
Cholestanol: 3.53
Desmosterol: 1.33
Hello I am interested in knowing whether LDL – P can be lowered without medication. My total cholesterol is 218. Triglycerides are 66. Total LDL cholesterol 129.total HDL cholesterol 75 non-HDL cholesterol 143 LDL – P1408 is there something I can do to lower the LDL – P without medication
I am unable to find any information regarding my husband’s situation. He has LDL-P 1387, LDL-C 131, HDL-C 38, HDL-P 27.9, TG 96, TC 188, LDL size 20.6. He exercises regularly (3x/WK), follows a low carb, high protein diet and has lost 60 lbs over the last year. Any ideas out there?
These are my numbers, HDL Cholesterol 96 mg/dL >39 mg/dL
Triglycerides 59 mg/dL 0 – 149 mg/dL
Cholesterol, Total 288 mg/dL 100 – 199 mg/dL
HDL Particle No, NMR 39.8 umol/L >=30.5 umol/L
Small LDL-P <90 nmol/L 20.5 nm
Because of my high HDL and small LDL-P, I feel comfortable not taking any statins, is this a wise choice? I am 5’3″, 104 lbs, 54 years old, eat very healthy and workout daily, both with weights and cardio activity.
I am 59, 5ft 6 , 117 lbs- I recently had 3 blockages, with only 1 mild chest pain to clue me in…. I was 132 lbs at the time. I am very active, physical job etc, I never felt bad.- after 3 heart test, a heart cath was what discovered the blockages. A stent was put in only on one that was 98% blocked, then sent home on statins. The statins about killed me from shoulder arm pain,muscle atrophy and even tore my bicep doing my first rotation with a jump rope for cardiovascular exercise.(surgery soon for that) my physician took me off statins and ran blood work 3 months later- I still exercise and eat 20-30 grms of jalapeno pepper daily. I dont know if that is what contributed to the cholesterol drop but the total was 159 which was a big drop for me .. The Triglycerides were 80. My heart doc put me on zetia to drop it slightly more… my general physician says that the blood work was still considered bad for an individual with 2 remaining blockages as my LDL particles were 1300…. He wants me to take shots every 2 weeks for cholesterol , that cost 14000 annually. what the crap? I want to gain weight as my weight has dropped to 117 .. as i exercise and try to watch my cholesterol intake….. how can I gain weight without affecting my LDL or bad cholesterol levels?
Lamont–Sorry for your troubles, but you sound motivated and hope you come out of this really fine.
First, regarding statin problems, I’m an expert, sad to say. See statinvictims.weebly.com for photo. Statins can trigger permanent neuromuscular diseases in those genetically predisposed. What you describe sounds like how my nightmare started, but who knows? Only 1% of adverse drug effects are ever reported.
Regarding the $14,000 drugs, they are indeed shown to lower LDL. But they are not shown to lower heart attacks, strokes, etc. The adverse effects–unknown, since these are new drugs. The exploitative adverse economic effect was predictable: drug companies are unscrupulous.
Read Peter C Gotzsche’s Deadly Medicines, winner of BMA first prize award.
All would be so much easier if adverse effects were reported!
thanks for your reply and info David…I am considering not going the route of the shots…anxious to see in 3 months how the blood work comes out…How long have you been dealing with the after effects of the statin? Is there hope of a recovering strength and muscle back?
Four years now. It’s progressive, so it gets worse and worse. At 68 I was trekking in the Himalayas, could jump in the air and kick over my head. At 69, after 7 months on 20 mg simvastatin, I couldn’t walk around the block. My old self was murdered for money–literally.
Not sure this will reach you. I have been LCHF for 6 months. Just had labs done. Stats: 48f/5’8″/152 lbs. Work out 5 days a week (Orange Theory Fitness)
Previous (no NMR done) 4/3/17:
Total: 231
LDL 138
VLDL 13
HDL 80
Tri 64
Current 2/24/2018
Total: 688
LDL-C: 586
HDL-C: 72
Tri: 150
LDL-P > 3500
HDL-P (Total) 32.2
Small LDL-P <90
LDL Size: 23.0
As you can see, a tremendous rise in LDL and Triglycerides. I seem to have ALOT of particles, yet not a lot of small ones (if I am reading right). So the doctor wants me on statins, but I am inclined not to take them. I don't know if any of this is a sign of increased risk of CVD, or if I need additional tests to check something else. I seem to be one of the few that the low-card diet grossly increases levels. Any thoughts or suggestions?
I’m a 71 year old female. Non smoker, treated Hashimoto’s, eating a gluten-free relatively low carb but high fat diet (butter, coconut oil, olive oil, pastured meats eggs & dairy, nuts, sardines, natto). Most carbs from vegetables and fruits (often berries). No prescription medications except Armour Thyroid. 5’4″ and currently weighing about 137 (haven’t worked off the holiday goodies yet). I usually weigh around 130.
TC: 285
LDL-C: 182 (Friedewald); 150 (Iranian)
HDL-C: 91
TG: 60
LDL-P: 1542
HDL-P: 38.3
Small LDL-P: <90
LDL-P size: 21.7
My ratios are off the charts, but I'm curious about the high LDL-P relative to my triglycerides. I don't have an IR score, but I'd be surprised if this were a problem given my lowish carb diet and low TG. I occasionally test for blood sugar just to know, and it's never been high, and I know it correlates with TGs anyway. Can you think of an explanation for the high LDL-P?
Also, is a high HDL-C value always a good thing?
Thank you.
Not certain if this thread is still active. If it is, I’m a 60 y.o female, never smoked with family history of CAD. My LDL-P came back elevated at 1207, LDL-C is 126, HDL-C is 67, Triglycerides 66, Total Cholesterol is 203, HDL-P is 30.4 and hsCRP (Cardio CRP) is 4.0. I have a coronary artery calcium scoring test later this week to determine if statins are right for me. I’ve lost 20 lbs in the past 6 months, but BMI at 28.5 so still overweight but getting better. I try to eat primarily vegetarian or fish only. Occasionally chicken, but no beef, lamb, pork or veal. And I try to stay with low carbohydrates. Any thoughts on if these numbers require statin therapy? Grateful for any insights anyone is willing to share!
Hi Jo-Ann
I would be curious to see the coronary calcium score before deciding on statin therapy. Your future risk for cardiac events is low if the calcium score is zero in which case statins could clearly be avoided in my opinion.
You might want to take a look a this blog post here.
The article contains a mistake, claiming LDL-C to be measured in mg/ml when actually it’s mg/dl.
Hello, and thank you in advance for your enlightenment in regards to my numbers below.
I’m very confused and scared after receiving my NMR test results. I’ve been following a Keto diet for the last 2 years (strict the first year, LCHF in the last few months). I have insulin resistance and am overweight. I lost 85 lbs on Keto, but I’m still over 200 lbs. Here are my results:
I’m 53, F, non smoker.
Thank you so much for your help.
Hi, I’m 39. 175cm height and 74kg weight.
My last NMR analisis:
CT: 386
LDL: 304
HDL: 70
TG: 44
NO-HDL: 316
LDL-P: 2635
LDL-P small: 839
LDL-P big: 473
LDL-P medium: 1323
should I have statins? Thank you