
Estimated reading time: 3 minutes
Measurements of lipids levels in blood are frequently used to assess the risk of future heart disease. The most commonly used measurements are total cholesterol, triglycerides and high density lipoprotein cholesterol (HDL-C). These numbers are then used to calculate low density lipoprotein cholesterol (LDL-C), which has been found to be strongly correlated with the risk of heart disease.

Recently measurements of atherogenic lipoprotein particles, such as LDL-P (LDL particle number), apolipoprotein B (apoB) and lipoprotein(a) have been found to be very useful to assess risk.
LDL-P measures the actual number of LDL particles (particle concentration). LDL-P may be a stronger predictor of cardiovascular events than LDL-C. Low LDL-P is a much stronger predictor of low risk than low LDL-C. In fact, about 30 – 40% of those with low LDL-C may have elevated LDL-P. Therefore you can have low LDL-C but still be at risk for heart disease, particularly if your LDL-P is elevated. Discordance is considered present if LDL-C differs from LDL-P.
LDL-C is a measure of the cholesterol mass within LDL-particles. LDL-C only indirectly reflects the atherogenic potential of LDL particles. ApoB and LDL-P on the other hand reflect the number of atherogenic particles, with no mention of cholesterol mass. ApoB and LDL-P are believed to be better risk predictors than LDL-C.
Many recent studies have looked into the importance of LDL-particle size. Studies show that people whose LDL particles are predominantly small and dense, have a threefold greater risk of coronary heart disease. Furthermore, the large and fluffy type of LDL may be protective.
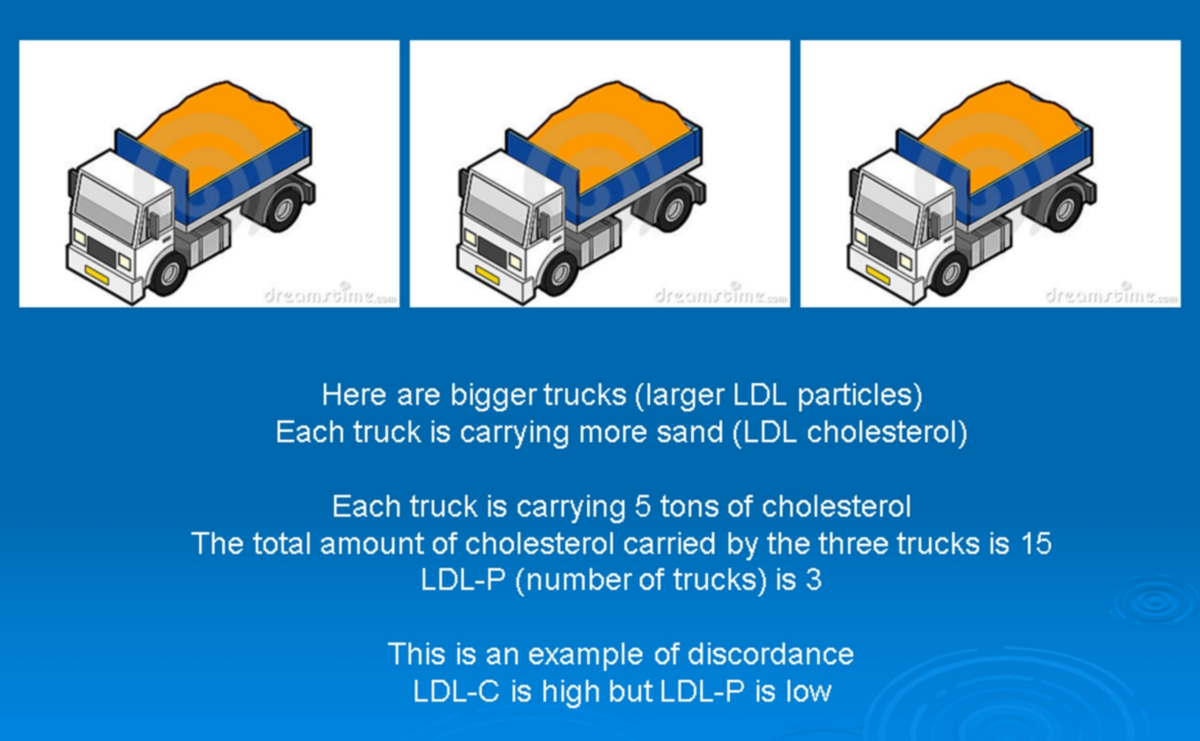
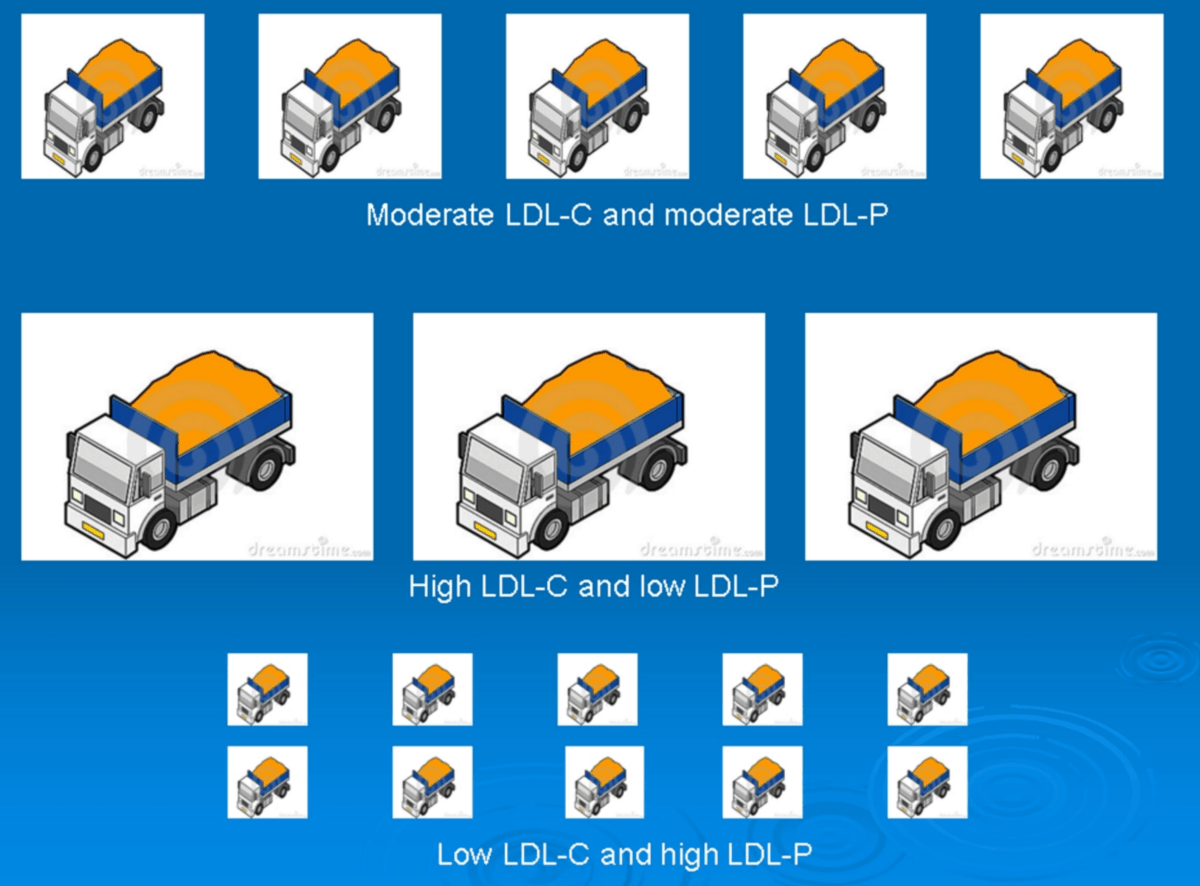
Sometimes it is difficult to understand the difference between LDL-C and LDL-P and how particle size comes into the picture. It is quite likely that LDL particle number and size will be used more often in the future to assess risk. Therefore I decided to share with you four slides I often use to simplify these issues. In the slides LDL lipoprotein is presented as trucks carrying sand (cholesterol).
Hope you enjoy the slides although you may find my chemistry to be on preschool level.


Discover more from Doc's Opinion
Subscribe to get the latest posts sent to your email.
As someone who’s own knowledge of chemistry is very much at the pre-school level I found this post and particularly the 4 slides extraordinarily helpful: Thank you.
Is the reason this is not used by most Drs yet is that there is no “pill” and thus no push from Pharma?
I think doctors don’t understand it. My Particle Number was 2500, My LDL was 250. I tell them this a discordance because the particle number is to high as compared to the LDL. My HDL is 90 – 100. several doctors have refused to give me the Advanced Lipid Test. They have tried to treat it with sttins. My LDL went done to 207… particle number remained high at 1500. The doctors all state the test is to expensive and they won’t order it. I’m not a doctor they should give a medical explanation as to why they don’t want to order it. The explanation would be currently -a group?- that makes theses decisions believes the regular LDL test catches reflects the particle number without taking the advanced test. I’ve explained to them I have a discordance they don’t get it. I had a pulmonary embolism last year I believe LDL-p had something to do with it.
I paid $99 for a complete cholesterol test through Life Extension. They also haveDr who will go over the test with you up to 30 minutes for free. They contract with Lab Corp to have the test done.
Hello my name is Tammy .I am very sorry to hear the unclear communication between you and the professional medical personnel.It is disappointing.I believe a patient has to be comfortable to communicate properly with a medical doctor or specialist or any one in the medical field .Also I believe it to be that a trained and experienced medical professional would be able to reconize this as to they are about taking care of another human being.With that being said have you called your insurance provider and inquired your self the expense of your health treatment and what test are available under your coverage plan .Sometimes getting a second opinion or diagnosis is good.Then you know what is available and another doctor could change the diagnosis if he orders the test. I wish many blessings upon you and your health .
Hi, Dr. Sigurdsson. You’ve got a very nice blog going here, mainly because of its two primary features: there is your medical expertise which oversees it all, plus the fact that it is not all about one-sided advocacy (especially with the diversity of commenters). That said, I don’t think that you would deny that you have an obvious leaning toward low carb – though I’m not quite sure if you favor that approach for everybody or instead mainly for the insulin resistant.
My aim is to try and discover what is best to do, so I have zero interest in being part of any ‘movement’ or engaging in the diet wars. (I have an Fx of CVD, but not much personal risk, AFAIK.) I’m not exactly a beginner, but I’m going farther now with trying to get a good overview of all the major studies on CVD prevention, as well as getting some practical insights from a practicing clinician. This looks like the best place to do that. So keep up the good work 🙂
Thanks KV. Appreciate your interest in my blog. Hope you continue visiting and feel free to share your thoughts 🙂
Hi, Jerry. Logically, the opposite would be true. As the result of advanced lipid testing, some people would get reclassified to a higher risk category. If those people cannot or will not lower their LDL-P through lifestyle changes, they might very well be put on statins and/or other meds.
Statins do lower LDL-P – just generally not as much as they lower LDL-C. Apparently, niacin might also lower LDL-P (because it lowers triglycerides); but as far as I know the OTC fast-acting niacin is safer on the liver than the prescription slow-acting Niaspan.
A standard lipid panel here costs around US$30, while the NMR test for LDL-P has been dropping and is around $75 now.
I’m a 54 year old male, 6’1″ and 225lbs. A recent physical revealed results that had my doctor prescribe statins. I have read very detrimental information and have resisted. Apart from the cholesterol numbers, I’m a picture of God health and eat a LCHF diet.
Here are my numbers age results from a website that does a basic calculation:
Your Total Cholesterol of 244 is HIGH RISK
Your LDL of 162 is HIGH RISK
Your HDL of 65 is OPTIMAL
Your Triglyceride level of 85 is NORMAL
RATIOS:
Your Total Cholesterol/HDL ratio is: 3.75 – (preferably under 5.0, ideally under 3.5) GOOD
Your HDL/LDL ratio is: 0.401 – (preferably over 0.3, ideally over 0.4) IDEAL
Your triglycerides/HDL ratio is: 1.308 – (preferably under 4, ideally under 2) IDEAL
LDL-P: 2048
HDL-P: 43.9
Small LDL-P: 856
LDL Size: 21.0
I’ve decided to once again put off the statins as a physical 2 years ago produced similar results and I’ve stayed statin-free.
Any thoughts on this?
So…I know this is incredibly uneducated but how to I get large an fluffy from small and dense?
p stratos
It depends on many things. If you’re overweight or have metabolic syndrome you could target the TG/HDL-cholesterol ratio.
I’m guessing no one has read this study:
https://www.athero.org/commentaries/comm564.pdf
I am guessing you didn’t check to see her ‘donations’ or what the two companies that gave them, sell?
https://projects.propublica.org/docdollars/doctors/pid/355934
If anyone can help out, would be greatly appreciated… since I been on a Ketogenic Diet.. my Apolipoprotein B went up to 230, and my lipoprotein (a) is at 99, what am I doing wrong, am I consuming too much Saturated Fats.. is it the grass fed butter, or the Caprilic Acid C8 from Brain Octane…
Maurice
Dietitian Franziska Spritzer wrote an interesting article on her blog explaining how her lipids, in particular LDL-C and LDL-P reacted to a LCHF/ketogenic diet https://www.lowcarbdietitian.com/blog/lipid-changes-on-a-very-low-carb-ketogenic-diet-my-own-experience
And a case report from some years ago
https://www.docsopinion.com/2013/07/24/low-carb-and-cholesterol/
speaking from personal experience — my spouse can eat like you and his cholesterol and BP remain optimal. If I even look at a hamburger, mine goes up, it has never been optimal. It’s your genetics.
I eliminated all cheese from my diet and began taking Cholest-off (an OTC plant stanol), and now consume under 10 grams of saturated fat a day. Use Fitday.Com (it’s free) and you’ll see it. I got my numbers down and put off statins for another year. PS your ideal # goes down as you age. I’m 66.
After major research, and read over 20 + books… I think I finally found an answer. that I am looking to get done this weekend… I think when the liver makes bile, the bile should be stored in the gallbladder (1L a day). but if your gallbladder has gallstones(cholesterol Stones) it prevents it from working properly and or holding enough bile to be used when you consume food, and specially fat.. I think thats why my cholesterol levels keep increasing dramatically every time I consume fat… and its taking a very long time to lower it… I will do a liver and gallbladder flush and see what happens.. keep you updated… As the Ultra sound scan does not show any stones in the liver nor the gallbladder…
Hi Maurice…any updates on this? Did the liver and gallbladder flush help with the cholesterol levels?
Thanks!
After the flush. Cholesterol LDL was a bit high but had gone down 20 points. So I increased my magnesium and vitamin c and only ate one protein meal a day with the secondary meal being 3 plates of cooked organic zucchini and 3 weeks and increased probiotics with every meal my cholesterol dropped from being as high as 10.3 down to 4.2 the doctor was shocked . So now for the past 4 weeks I increased the fats again to see if it was the fats or my gallbladder is clean and blood is stable.
Dr. Sigurdsson, just came upon this site. It’s fascinating, thank you. I’m a 66 year old male who, until recently, thought he was pretty healthy. I always knew my total Cholesterol number was elevated-It’s currently 260. My doctors had always said though that the hdl/ldl ration was good and not to worry. So I didn’t worry. A recent series of tests including a CAT scan indicated that I have some moderate blockage in and a cardiologist wants to put me on statins.
The calcium test has these numbers: Left main=34,
Left Anterior Decending=61
Left Circumference=75
At this point i’m reluctant to begin taking a drug that has as many negative affects as positive in my opinion. I just learned about the small vs large ldl particles but this was not part of the latest blood test. the numbers I have are:
Triglicerides-94
LDL-151
HDL-90
Cholesterol/HDL Ratio-2.9
TSH Ultrasensitive- 1.530
Free T-4 – 6.2
T-3 Uptake _ 35.6
T-3 Total -0.82.
Trigliceride/ HDL Ratio is-1.04.
With these numbers I dont know what my next step should really be. I did start a Vegan diet eliminating all meat,fish, dairy, and oils. It’s killing me. Could there be another option other than a lifetime of statin drugs and do you think this type of diet could reduce the blockage?
Hi Jerry
The TG/HDL-C ratio is relatively benign suggesting that it’s unlikely that you have insulin resistance or a small LDL-pattern.
https://www.docsopinion.com/2014/07/17/triglyceride-hdl-ratio/
Looking only at your lipid numbers I would probably not suggest statin treatment. However, your coronary calcium score is just above median for your age suggesting that you may be at slightly increased risk. Some doctors will recommend statins in this situation.
But, although statins may reduce risk to a slight extent, healthy lifestyle is the most important thing in my opinion. Furthermore, some people experience side effects from statins. But, it’s a choice you have and should discuss with your doctor.
https://www.docsopinion.com/2014/08/19/coronary-calcium-score/
I would suggest a real food diet with lots of vegetables, fresh meat and fish. I recommend avoiding sugars and refined carbs, and refined foods in general. I’m not afraid of healthy natural fats, cheese, avocado, eggs, olives and olive oil, nuts etc.
Dr., thank you for your speedy reply. As I seem to have, according to your own posting, moderate coronary artery disease:
(“Coronary Calcium Score Interpretation
Based on a number of studies, the following definitions are used to
relate the coronary artery calcium score to the extent of
atherosclerotic coronary artery disease:
Coronary calcium score 0: No identifiable plaque. Risk of coronary artery disease very low (<5%)
Coronary calcium score 1-10: Mild identifiable plaque. Risk of coronary artery disease low ( 400: Extensive atherosclerotic plaque. High likelihood of at least one significant coronary narrowing.”)
A cardiologist said that I have coronary disease with the calcium score of 170. I shared the information and concerns about a life taking statins with my family doctor and he suggested I look in to the research of the Drs Esselstyn and Ornish. The diet I began a month ago, was developed by Dr. Caldwell Esselstyn and also, with some modification, by Dr. Dean Ornish. I have always had what I thought was a good diet- In fact, your dietary suggestions to me is almost exactly the way I’ve been eating most of my life. I’m 66 and have always weighed around 150 pounds. These doctors frown on ANY oil at all and in fact, their mantra is eat nothing with a mother or a face- including eggs. Doesn’t leave much. IN fact, I have already lost about 5 pounds and don’t feel that I have the energy or that I am getting the protein I need in my diet even with the beans and legumes.So, once again, with the numbers I quoted above, is there another test that would offer a more detailed analysis of my specific plaque issue or a known way to reduce the plaque itself without the use of statins. I could not get a consultation appointment before mid August with a cardiologist so I appreciate your input and your time. Your site is fascinating. Thank you again. Jerry Knaster
Jerry, Alex is not going to have your heart attack for you. You are. The cardiologist that told you about going on a Whole Food Plant Based lifestyle change (as low in all fats as possible- more a little later) is telling you the truth. In that way there is the possibility of decreasing the size of the atherosclerotic plaques already built up in you coronary arteries that are, quite literally, going to kill you if you don’t begin to take action soon. You don’t really have to worry about not getting enough protein as your body is very efficient with recycling the amino acids the your body needs to stay healthy. The nuts/legumes/nuts that will become part of your lifestyle will provide you with the essential amino acids that you may fall short of. Realistically proteins need not be more than 5% of your caloric intake. Go to the “Forks over Knives” website for inspiration and recipes to make eating interesting. [No I have no affiliation.] I’m talking about a lifestyle change here Jerry because the scientific evidence is staring you in the face. You have been mistaken believing that you have been eating a healthy diet; if you stick with it it will be your death-style, like so so many people. You will need to take in a very small amount of fats in order to absorb Vitamins A, D, E, and K. At 66 you want to make sure that Omega 3’s make up some of that fat. If you don’t want to lose weight increase the number of calories of either by eating more resistant starch, or fruits and vegetables with fiber added to help with satiation. This will help with the feeling of not enough energy.
Alex’s stroking your ego by telling you that your coronary calcium score is just above the median is a moot point because the calcium found in the atheroma is not what will kill you. If your current cholesterol is 260, what has it been for the last 45 years? That is why you are in the situation you find yourself in now. It is cholesterol that makes of the majority of the structure of the atheroma and once it become supersaturated it will crystallize and those crystals will pierce the epithelium of the artery; this will set of the wound healing mechanisms of the body in motion within the artery causing a thrombosis to form, cutting off the blood to all down stream myocardial tissue. And damage done will depend on where specifically this happens along that artery; and remember your percentages of blockage here Jerry; this is not an if situation here it’s a when in your case. Make the change. I won’t quote the research papers because I’m not going to get into a my scientific studies are better than your scientific studies argument with Alex.
Jerry,
Alex is not going to have your heart attack for you. You are. The
doctor that told you about going on a Whole Food Plant Based lifestyle
change (as low in all fats as possible- more a little later) is telling
you the truth. In that way there is the possibility of decreasing the
size of the atherosclerotic plaques already built up in you coronary
arteries that are, quite literally, going to kill you if you don’t take
action. You don’t really have to worry about not getting enough protein
as your body is very efficient with recycling the amino acids the your
body needs to stay healthy. The nuts/legumes/beans that will become part
of your lifestyle will provide you with the essential amino acids that
you may fall short of. Realistically proteins need not be more than 5%
of your caloric intake. Go to the “Forks over Knives” website for
inspiration and recipes to make eating interesting. [No I have no
affiliation.] I’m talking about a lifestyle change here Jerry because
the scientific evidence is staring you in the face. You have been
mistaken believing that you have been eating a healthy diet; if you
stick with it it will be your death-style, like so so many people. You
will need to take in a very small amount of fats in order to absorb
Vitamins A, D, E, and K. At 66 you want to make sure that Omega 3’s make
up some of that fat. If you don’t want to lose weight increase the
number of calories either by eating more resistant starch, or fruits and
vegetables with fiber to help with satiation. This will help with the
feeling of not enough energy.
Alex’s stroking your ego by telling
you that your coronary calcium score is just above the median is a moot
point because the calcium found in the atheroma is not what will kill
you. If your current cholesterol is 260, what has it been for the last
45 years? That is why you are in the situation you find yourself in now.
It is cholesterol that makes up the majority of the structure of the
atheroma and once it become supersaturated it will crystallize; those
crystals will pierce the epithelium of the artery; this will set of the
wound healing mechanisms of the body in motion within the artery causing
a thrombosis to form, cutting off the blood to all down stream
myocardial tissue. The damage done will depend on where specifically
this happens along that artery; and remember your percentages of
blockage here Jerry; this is not an if situation here it’s a when in
your case. Make the change. I won’t quote the research papers because
I’m not going to get into a my scientific studies are better than your
scientific studies argument with Alex.
Hi Jerry, what side statin side effects are you worried about? I was a bit on the fence myself for years, however no diet helped lower cholesterol (in my case, it is genetic). I’ve been now taking for 7 or so years without any noticeable side effect.
Studies show that 50-70% of men have their first heart attack before they have any chest pain. There are two issues with the traditional treatment of LDL cholesterol. First, many people experience adverse effects with statin therapy, requiring alternative approaches via diet and supplements to get their LDL cholesterol levels under control. The second issue is LDL cholesterol evaluation. We need to be looking at LDL particle number and size as well as whether or not it’s been modified. LDL cholesterol modification can cause inflammation, oxidative stress, and finally vascular immune dysfunction. In this talk, Dr. Houston explains that if we can implement a targeted nutrition approach that attacks the mechanism by which LDL cholesterol causes atherosclerotic plaque development, we’re more likely to prevent a heart-related clinical event.
Well said, Mark. The root of atherosclerosis lies in chronic systemic inflammation. The mainstream medical community has been barking up the wrong tree for 60 years, in my opinion.
Doctors have tried to treat it with Statins. My LDL went done to 207… particle number remained high at 1500. The doctors all state the test is to expensive and they won’t order it. I’m not a doctor they should give a medical explanation as to why they don’t want to order it. The explanation would be currently -a group?- that makes theses decisions believes the regular LDL test catches reflects the particle number without taking the advanced test. I’ve explained to them I have a discordance they don’t get it. I had a pulmonary embolism last year I believe LDL-p had something to do with it.
Hi,
Thanks for your post. Would you be able to provide any insight into a situation where my LDL-P is higher than my LDL-C, but my LDL pattern is A.
LDL-P: 1827
LDL-C: 136
I have high LDL (1804), high LDL Small (284) and high LDL Medium (438) particle numbers. LDL Pattern is “A” and LDL peak size is slightly elevated (220.5 Angstorm). HDL Large particle numbers are in moderate range (6084). My LDL was found to be not oxidized. My Ca score was 468 in 2014. I cannot tolerate statins or repatha. How significant non-oxidized LDL is in preventing heart attack and stroke when LDL particle numbers are all high?