
Estimated reading time: 11 minutes
In cardiovascular medicine, some numbers are sacred. LDL-cholesterol (LDL-C) has long been the cornerstone of risk assessment and treatment targets. But what if we’ve been following the wrong number?
This updated article revisits and expands on a piece I wrote in 2021 — enriched by new evidence, deeper clinical insights, and a clearer understanding of risk. What hasn’t changed is the central message: ApoB matters.
Apolipoprotein B (ApoB) — a protein carried on every atherogenic lipoprotein particle — may be a better predictor of cardiovascular risk than LDL-C, non-HDL-C, or total cholesterol. In fact, it directly reflects the number of atherogenic particles in circulation — each one capable of triggering atherosclerosis.
Let’s unpack why this number deserves more attention — in the lab, in the clinic, and in the exam room.
Atherosclerosis Begins With a Particle
Atherosclerosis — the buildup of plaque in the arteries — starts early and silently. It happens when certain fat-carrying particles in the blood, especially those containing ApoB, get stuck in the artery wall. That event sets off a chain reaction: the immune system responds, white blood cells move in, and inflammation begins.
These white blood cells gobble up the trapped particles and turn into foam cells, which help form fatty streaks — the early signs of plaque. Over time, the buildup grows and the artery narrows, limiting blood flow. But the real danger comes if the plaque ruptures. A blood clot can form suddenly and block the artery completely, causing a heart attack or stroke.
ApoB is present on every one of those harmful fat-carrying particles. So, by measuring ApoB, we’re not just guessing at risk — we’re counting the very particles that start the disease process.
Lipoproteins: The Carriers of Risk
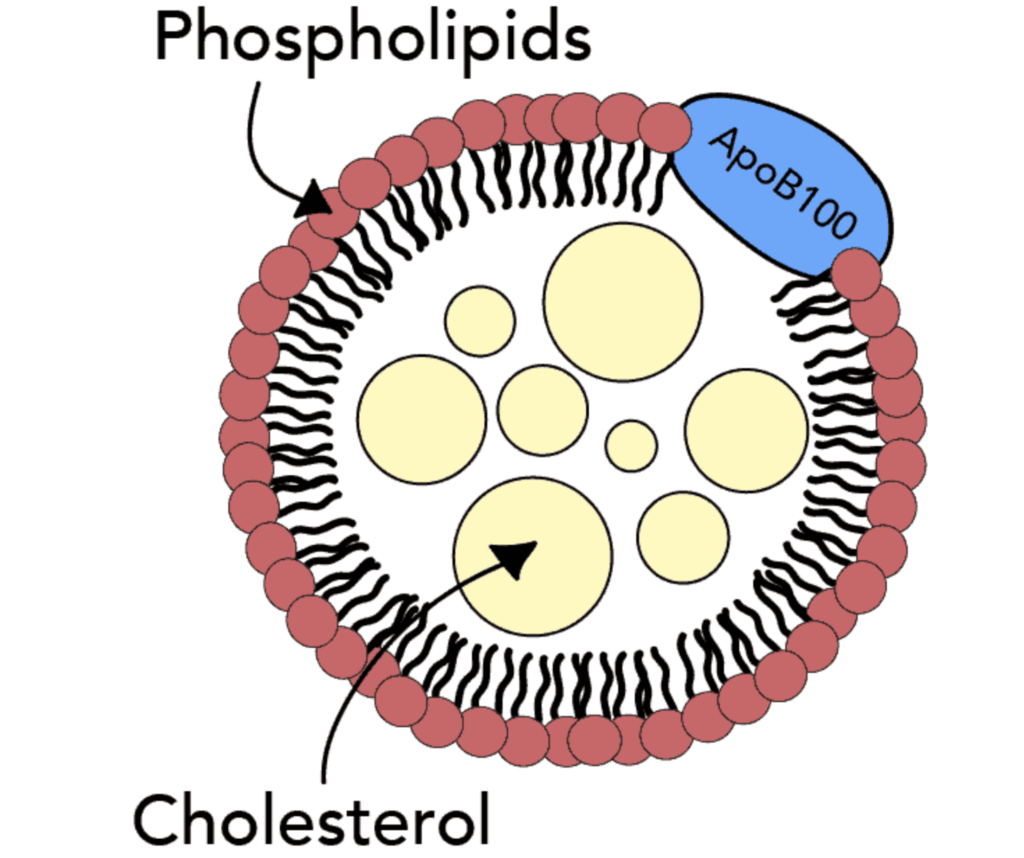
Fats are insoluble in water. To travel through the bloodstream, they need packaging. That packaging is the lipoprotein — a small sphere made of proteins and lipids that carries cholesterol, triglycerides, and phospholipids to different parts of the body.
There are several classes of lipoproteins, each with a different role and impact on health:
-
Chylomicrons — carry dietary fats from the intestine to tissues.
-
Very-low-density lipoprotein (VLDL) — deliver triglycerides made by the liver to the tissues.
-
Intermediate-density lipoprotein (IDL) — a transitional form between VLDL and LDL.
-
Low-density lipoprotein (LDL) — often called “bad cholesterol,” it delivers cholesterol to tissues and can contribute to plaque buildup.
-
Lipoprotein(a) [Lp(a)] — a genetically influenced particle that is particularly atherogenic.
-
High-density lipoprotein (HDL) — the so-called “good cholesterol,” involved in reverse cholesterol transport.
Only the first five lipoproteins contain ApoB and are considered atherogenic — capable of penetrating the artery wall and triggering atherosclerosis. HDL does not carry ApoB; instead, it contains ApoA-I, which is believed to help protect against plaque formation.
Understanding which particles carry cholesterol — and how many of them are present — is more informative than simply knowing how much cholesterol is in the bloodstream. That’s where ApoB comes in.
ApoB: One Protein, One Particle
There are two main forms of apolipoprotein B:
-
ApoB-100, synthesized in the liver, is present in VLDL, IDL, LDL, and Lp(a) particles — all of which are considered atherogenic.
-
ApoB-48, synthesized in the intestine, is found in chylomicrons, which are responsible for transporting dietary fats but are generally not involved in plaque formation.
From a cardiovascular standpoint, ApoB-100 is the key player. Each atherogenic particle carries a single ApoB-100 molecule. That means the concentration of ApoB in the blood provides a direct measure of the total number of atherogenic lipoprotein particles. It’s not an estimate — it’s a count.
This is important because traditional markers like LDL-C do not measure particle number; they measure how much cholesterol is carried within LDL particles. But LDL particles can vary in size and cholesterol content. Two people with the same LDL-C could have very different numbers of particles — and therefore different levels of risk.
This mismatch between LDL-C and particle number is known as discordance. It’s more than just a lab curiosity — it has real consequences for diagnosis and treatment. Patients with discordantly high ApoB are at greater risk, even if their LDL-C appears acceptable. Ignoring that difference could mean missing an opportunity for prevention.
LDL-C vs. ApoB: When the Numbers Don’t Agree
Imagine two patients. Both are in their mid-50s, both are non-smokers, and both have an LDL-C of 110 mg/dL. On the surface, they look similar — maybe even reassuringly average. But under the hood, things are very different.
One patient has small, dense LDL particles — the cholesterol cargo in each is modest, but there are many of them. The ApoB level is high. The other has large, cholesterol-rich LDL particles — fewer in number, and the ApoB level is low. Same LDL-C, very different particle counts. And very different risks.
The first patient’s arteries are quietly under siege. More particles mean more chances to penetrate the arterial wall and start the atherosclerotic process. The second patient? Not risk-free — but likely far safer.
The evidence backs this up:
-
ApoB correlates more strongly with cardiovascular events than LDL-C or non-HDL-C.
-
Discordance between LDL-C and ApoB is especially common in people with metabolic syndrome, insulin resistance, or type 2 diabetes.
-
Many statin-treated patients reach LDL-C targets, but their ApoB remains elevated — and with it, their residual risk.
“It’s not the cholesterol content, but the number of delivery vehicles that drives the risk.”
And it’s not just LDL particles. ApoB is carried by all atherogenic lipoproteins — including VLDL (which transports triglycerides), IDL (a transitional remnant), Lp(a) (a genetically inherited risk factor), and remnants of chylomicrons. Each of these particles carries one ApoB-100 molecule, and all can contribute to plaque formation.
So when you measure ApoB, you’re not just measuring LDL. You’re capturing the full spectrum of atherogenic lipoproteins — a more complete view of the forces that drive atherosclerosis.
ApoB in the Guidelines
It’s taken time — and no shortage of evidence — but the tide is turning. What was once an “advanced lipid marker” tucked away in specialist clinics is now moving to center stage. Guideline committees, expert panels, and frontline clinicians are all beginning to agree: ApoB isn’t optional anymore. It’s essential.
The European Society of Cardiology (2023) led the way, recommending ApoB as the preferred metric when available. They also set clear treatment thresholds: less than 80 mg/dL for high-risk patients, and under 65 mg/dL for those at very high risk.
The Canadian Cardiovascular Society (2021) followed suit, naming ApoB the preferred secondary target after LDL-C. Meanwhile, the American Heart Association (2024 Science Advisory) emphasized ApoB’s value in patients with cardiometabolic risk — especially in those discordant cases where LDL-C looks fine on paper but risk remains high.
Then came the push forward.
In 2024, the National Lipid Association (NLA) published an expert consensus declaring ApoB a “clinically actionable tool.” They recommended it not just for academic curiosity but for practical use — particularly in patients with metabolic syndrome, diabetes, elevated triglycerides, or existing atherosclerotic disease.
By 2025, the ripple had become a wave. Proposed guideline updates suggested that ApoB levels above 120 mg/dL (1.2 g/L) may warrant statin therapy in intermediate-risk individuals, even when LDL-C appears to be in a so-called ‘normal’ range.
One editorial in a leading lipidology journal put it bluntly: “ApoB has moved from optional to essential.”
Still, many clinicians haven’t caught up. Routine ApoB testing remains underused — not because it lacks value, but because inertia lingers. The cholesterol-centric mindset is hard to shake.
But the evidence keeps piling up. And the message is now hard to ignore: if you want to assess risk — and truly reduce it — count the particles, not just the cholesterol they carry.
How to Interpret AboB
Typical reference range: 40–125 mg/dL
While the reference range offers a general sense of what’s normal, clinical context is key. ApoB levels should always be interpreted in light of an individual’s total cardiovascular risk profile — including age, family history, metabolic health, and other lipid markers.

Because each atherogenic lipoprotein carries exactly one ApoB molecule, measuring ApoB is effectively counting the number of particles capable of causing harm. And thanks to standardization across labs and its independence from fasting status, it’s now easier than ever to use ApoB testing in clinical practice.
For patients and clinicians alike, ApoB provides clarity where cholesterol measurements may confuse — a direct signal, rather than an indirect estimate.
ApoB and Lifestyle: What Helps
There’s no single diet or magic fix for ApoB — but there are powerful levers we can pull. Because ApoB reflects the number of atherogenic lipoprotein particles, lifestyle interventions that reduce metabolic stress or improve lipid handling can have a direct effect.
Interventions that may lower ApoB:
-
Carbohydrate restriction, especially in insulin-resistant or metabolically unhealthy individuals, can reduce the liver’s overproduction of VLDL particles — a major contributor to elevated ApoB.
-
Weight loss, particularly visceral fat loss, reduces systemic inflammation and improves insulin sensitivity, both of which can lower ApoB.
-
Regular exercise — not just for burning calories, but for improving muscle insulin uptake and reducing hepatic fat — can favorably shift the ApoB/ApoA-I ratio.
-
Dietary shifts away from industrially produced fats and processed carbohydrates may lower ApoB even in the absence of weight loss.
It’s important to note that some interventions may lower LDL-C while leaving ApoB unchanged — a reminder that our goal is not just to move numbers, but to reduce risk.
Pharmacologic therapies that reduce ApoB:
-
Statins — first-line agents that reduce cholesterol synthesis and lower both LDL-C and ApoB.
-
Ezetimibe — works by blocking cholesterol absorption; can be additive to statins in reducing ApoB.
-
PCSK9 inhibitors — highly effective at lowering both LDL-C and ApoB, particularly useful in very high-risk patients.
-
Bempedoic acid — modest LDL-C and ApoB reductions, with utility in statin-intolerant patients.
-
Fibrates — particularly helpful in those with elevated triglycerides; may reduce ApoB by improving particle clearance.
Lifestyle and pharmacology are not separate paths — they’re complementary tools. And both can be guided more precisely when we know the particle count, not just the cholesterol content.
The Bottom Line: It’s Time to Rethink Risk
We’ve come a long way since the cholesterol-centric view of heart disease. ApoB offers a clearer lens: it counts the particles that do the damage, not just their cargo.
For patients: Ask your doctor if measuring ApoB makes sense for you.
For clinicians: In cases of discordance, residual risk, or metabolic dysfunction, ApoB often tells the real story.
Because in cardiovascular prevention, the most dangerous number… may be the one we’ve been ignoring.
Related Reading on Doc’s Opinion
- The 12-Step Biology of Atherosclerosis (link)
- Non-HDL Cholesterol: The Hidden Heart-Disease Predictor You’ve Overlooked (link)
- Atherogenic Dyslipidemia (link)
- When High LDL Leads to Heart Disease — And When It Doesn’t (link)
- The Triglyceride/HDL Cholesterol Ratio (link)
- LDL-C vs. LDL-P: What’s the Difference? (link)
- What’s the Best Lipid Marker to Predict Risk? (link)
- High Triglycerides — And How to Lower Them (link)
- VLDL, Triglycerides & Remnant Cholesterol (link)
- HDL Cholesterol — The Good, the Misunderstood (link)
- 10 Pitfalls of Using LDL-C to Assess Risk (link)
- The Role of Low-Density Lipoprotein (LDL) in Atherosclerosis and Heart Disease (link)
- LDL Particle Number vs. Size — Made Easy (link)
- LDL-P (link)
-
Lipoprotein(a): The Overlooked Particle That Most Cholesterol Tests Miss (link)
References
- Sniderman AD, Thanassoulis G, Glavinovic T, et al. Apolipoprotein B Particles and Cardiovascular Disease: A Narrative Review. JAMA Cardiol. 2019;4(12):1287–1295.
- Ference BA, Kastelein JJP, Ray KK, et al. Association of Triglyceride-Lowering LPL Variants and LDL-C–Lowering LDLR Variants With Risk of Coronary Heart Disease. JAMA. 2019;321(4):364–373.
- Borén J, Chapman MJ, Krauss RM, et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease: Pathophysiological, genetic, and therapeutic insights. Eur Heart J. 2020;41(24):2313–2330.
- Pencina MJ, D’Agostino RB, Larson MG, et al. Predicting the 30-year risk of cardiovascular disease: the Framingham Heart Study. Circulation. 2009;119(24):3078–3084.
- Mach F, Baigent C, Catapano AL, et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk. Eur Heart J. 2020;41(1):111–188.
- Anderson TJ, Grégoire J, Pearson GJ, et al. 2021 Canadian Cardiovascular Society Guidelines for the Management of Dyslipidemia. Can J Cardiol. 2021;37(8):1129–1150.
- Grundy SM, Stone NJ, Bailey AL, et al. 2018 AHA/ACC Guideline on the Management of Blood Cholesterol. J Am Coll Cardiol. 2019;73(24):e285–e350.
- Toth PP, Philip S, Hull M, Granowitz C.
- Addressing residual risk beyond statin therapy: New targets in the management of dyslipidaemias–A report from the European Society of Cardiology Cardiovascular Round TableJournal of Clinical Lipidology, Volume 18, Issue 5, e685 – e700. J Clin Lipidol. 2019;13(3):374–382.
- Stanisław Surma, Michael D. Shapiro, Maciej Banach, Breaking new ground in lipid management: Insights from the 2024 American College of Cardiology Scientific Sessions,Pharmacological Research,Volume 205,2024,107246,ISSN 1043-6618,https://doi.org/10.1016/j.phrs.2024.107246.
- Jacobson TA, Ito MK, Maki KC, et al. National Lipid Association Recommendations for Patient-Centered Management of Dyslipidemia. J Clin Lipidol. 2024;18(2):e1–e24.
- Sniderman AD, Williams K, Contois JH, et al. A Meta-Analysis of LDL-C, non-HDL-C, and ApoB as Markers of Cardiovascular Risk. Circ Cardiovasc Qual Outcomes. 2011;4(3):337–345.
- Wilkins JT, Li RC, Sniderman A, Chan C, Lloyd-Jones DM. Discordance Between Apolipoprotein B and LDL-Cholesterol in Young Adults Predicts Coronary Artery Calcification: The CARDIA Study. J Am Coll Cardiol. 2016 Jan 19;67(2):193-201. doi: 10.1016/j.jacc.2015.10.055. PMID: 26791067; PMCID: PMC6613392.
- Frost PH, Havel RJ. Rationale for Use of Non-HDL Cholesterol Rather Than LDL-C as a Target for Lipid Lowering Therapy. JAMA. 1998;279(22):1642–1646.
- Behbodikhah J, Ahmed S, Elyasi A, Kasselman LJ, De Leon J, Glass AD, Reiss AB. Apolipoprotein B and Cardiovascular Disease: Biomarker and Potential Therapeutic Target. Metabolites. 2021 Oct 8;11(10):690. doi: 10.3390/metabo11100690. PMID: 34677405; PMCID: PMC8540246.
- Ramjee V, Sperling LS, Jacobson TA. Non-high-density lipoprotein cholesterol versus apolipoprotein B in cardiovascular risk stratification: do the math. J Am Coll Cardiol. 2011 Jul 26;58(5):457-63. doi: 10.1016/j.jacc.2011.05.009. PMID: 21777740.
- Sniderman AD, Dufresne L, Pencina KM, Bilgic S, Thanassoulis G, Pencina MJ. Discordance among apoB, non-high-density lipoprotein cholesterol, and triglycerides: implications for cardiovascular prevention. Eur Heart J. 2024 Jul 12;45(27):2410-2418. doi: 10.1093/eurheartj/ehae258. PMID: 38700053; PMCID: PMC11242442.
- Krauss RM. Lipoprotein Subfractions and Cardiovascular Disease Risk. Curr Opin Lipidol. 2021;32(4):197–204.
quote:
Atherosclerosis is initiated when an apoB-containing lipoprotein particle is caught in the vessel wall.”
The immediate questions must be: why (is it caught)? what (under what conditions)? how (it is caught (mechanism))?
why is nothing else apparently caught?
Thanks
That’s the million dollar question. We have to assume that many factors are involved; the status/permeability of the endothelium, the number of apoB containg particles, external facors like smoking, the presence of diabetes etc.
Sorry, I am slow to respond.
Is the initiating “event” an injury to the endothelium (ultimate cause).
Therefore, we need to understand that aspect first – there are potentially many causes (of injury) events.
To start with, perhaps a weakened endothelium due to “shortened” glycocalyx caused by a hi-carb diet?
Or perhaps low vitamin C levels.
Or as you imply many different things like smoking.
So the key question is:
Can the apoB-containing lipoprotein particle cause the injury or does this particle arrive on the scene subsequently (deliberately as part of the repair process or accidently?) ?
.
Axel,
Any thoughts on my questions?
.
Dr.- Within the factors you mention, given what I have read on the subject, the only one that seems to be beyond our control with either drug or behavioral modification is “status/permeability of the endothelium,” which I assume you mean the inner lining of arteries. Of all the issues with ApoB, it seems this is the most concerning. Where is medicine vis-a-vis its diagnostic ability to determine an objective status/permeability of the endothelium and more importantly, suggested remedy for diagnosed susceptibility to ApoB.
Always good reading Doc. Keep writing.
Thanks Neil
Great Content!
Since I am pretty much new to blog writing this was really helpful in understanding more about heart diseases and I’m really excited to dig deep more and curate valuable context.
Keep up the good work.
Great read and helpful, Thanks.
I’m already on 20mg rosuvastatin daily and adhere to a low-carbohydrate diet. My ApoB is still 116 and I don’t know what to do to lower it further.
No diabetes, BMI of 21, good waist/height ratio.
Typically, should the statin be increased or should a PCSK9 inhibitor be added?
I am also not sure about diet. I eat low-carb with a lot of vegetables. I don’t consume much saturated fat (a little from cottage cheese.) Is the low-carb or Esselstyn-type diet superior for this condition.
I have done a ton of research and I’m stuck at this point. It’s VERY frustrating.
Ms. Maarten-
I’ve had CD for years, asymptomatic responses to stress tests, stent implementation, and currently take 10mg crestor and 10mg Ezetimibe. I make sure to have protein with every meal and try to keep my diet in check. I’m not afraid of dairy or occasional red meat. After all, my blood type is O+. Like you, I do not suffer from other diseases. My numbers are cholesterol 113, LDL 38 and Apob 49. I attribute much of that numbers success to meds and diet but I believe I’ve only been able to achieve them, along with good health, with a vigorous exercise program I’ve maintained for 40+ years. I exercise heavily at least 3X per week, incorporating resistance (weight) for 45 minutes, 20 minutes of intense aerobics (twice resting heart rate) and stretch/relaxation for 20 minutes. As a male, loss of muscle mass is always an issue and I believe that resistance training aids in slowing that process. I think that’s important for females, too. I’m now 75 and able to maintain my training regimen and active life, even with arthritis. In fact, I think muscle support for my joints through resistance training is an anti-arthritis remedy. I’m not fat, not overweight, and don’t have, as Arnold would say, “girly, old man arms.” I say this because I did not see anything in your remarks regarding regular, intense exercise. While my BMI may be 25-26, it is the result of muscle mass rather than fat. And when I say aerobic exercise, I don’t mean walking on a treadmill and reading with headphones on. If you are exercising at a sufficient intensity, you should have trouble talking and should be breathing heavily. I would be interested to hear from you in six months if you initiate a solid exercise program. I’d bet you would be very happy with your ApoB results…good luck
I know I have contact with you again, but I highly recommend a book by Dr. Peter Attia: “Outlive” I guarantee you will not be disappointed! I’m 73 years old, former collegiate gymnast recovering from a heart attack in 2019 yeah. My numbers aren’t as good as yours and I know medication’s.
Try eliminating refined carbs, adding whole grains and legumes, and eliminating all meat, fish, dairy, and eggs from your diet. See https://nutritionfacts.org/ for a guide to a plant-based, whole food diet.
I’m in the same situation and would love an informed opinion. The Esselstyn diet seems highly unnatural. Though I am already 95% vegan, he takes it a step further by requiring nearly 0 fat, which would be very difficult for me to do. Curious about the value of doing this and whether it can help with those of us who have high Apo(b) but otherwise good health markers. Are there other options?
You can work with your doctor and try an Essylstein-type diet to see if it works. You can get blood tests regularly to see if it’s making it better or worse. The low-carb diet works for many, but it didn’t work for me.
You can also try a natural food Mediterranean style diet with whole grains, vegetables, legumes, fish, poultry, some red meat, nuts, olive oil, and some fruit. Staying away from anything with white flour, sugar, bread, salt, and processed industrial oils including corn oil, soybean oil, and canola oil. It’s this processed factory made food that will kill you.
I eat 90% of food this way. The only time I stray is when I eat out with friends, or if someone invites me over for dinner. For my own eating, I cut up fruit, make salads with romaine, carrots, onions, and bell peppers, steam vegetables, eat old fashioned rolled oats, brown rice, canned or baked salmon, chicken, steak, and other natural foods. When I had a heart condition, I started the a low-carb diet, and did for many years until my blood pressure and cholesterol numbers got too high. I’ve been eating this way, all my blood testing numbers are good, am am able to avoid statins and drugs, and it’s easier for me not to be overweight. The only difference with the way I eat and the Mediterranean is that I lay off olive oil and nuts. I read the Pritikin Program book, and it really opened up my eyes about eating for heart health. Similar to Essylstein, but around 3 oz fish or meat a day. On a vegan diet, it may be tough to get enough minerals, vitamins, AHA, DHA, and protein.
Doesn’t ApoB more or less track with particle size? When broken down by particle size, large and medium LDL particles have no association with heart disease, but small dense LDL particles are greatly associated. So isn’t ApoB basically just a proxy for Small-LDL-P? Kind of like triglyceride/HDL ratio is a proxy for particle size as well?
what AI had to say about your comment – “I’d say that statement is partly true, but oversimplified — and in some cases, misleading.
⸻
1. ApoB is not just a proxy for small LDL
• ApoB counts all atherogenic lipoprotein particles:
• LDL (small, medium, large)
• VLDL
• IDL
• Lp(a)
• Each particle, regardless of size, has one ApoB molecule.
• This means ApoB measures particle number, not size.
⸻
2. Particle size matters — but less than number
• Older thinking (pre-2010) was that small, dense LDL was the main villain.
• Large prospective studies (like the MESA and INTERHEART) show small LDL is harmful mostly because people with more small LDL tend to have more LDL particles overall.
• When you control for ApoB (particle number), particle size often stops being an independent predictor of heart disease.
⸻
3. Why the confusion?
• Small LDL-P and high ApoB often travel together:
• High triglycerides + low HDL → more small LDL particles → higher ApoB.
• This is why TG/HDL ratio can loosely predict particle size and often tracks with ApoB.
• But someone can have mostly large LDL particles and still have high ApoB — and still be at high risk, because the artery wall doesn’t care about particle size as much as how many particles are colliding with it.
⸻
4. Summary Table
Marker What it measures Heart disease prediction power
ApoB Number of atherogenic particles (all sizes) Strong, independent predictor
LDL particle size Distribution of large vs small LDL Weaker once ApoB is known
TG/HDL ratio Indirect proxy for insulin resistance & small LDL Useful shortcut, but not exact
⸻
💡 Bottom line: ApoB is not just a small-LDL proxy — it’s a direct measure of how many particles you have that can penetrate the arterial wall. Particle size can still give context, but for risk assessment, ApoB is generally more powerful and simpler.
⸻
If you’d like, I can show you a chart from MESA data that makes it visually clear why ApoB beats particle size for predicting heart disease. It’s pretty convincing.”
Tough when this test is rarely available. Low carb diets can increase LDL-C through legitimate processes – but LDL-P remains uncertain.
More sand, but how many trucks?
Thank you for this post.
Two questions- hasn’t it been shown that the body makes cholesterol irrespective of cholesterol ingested? Other dietary factors drive high cholesterol?
Second –
“The normal range for apoB is 40-125 mg/dL.”
I believe these numbers are normal for the American population- which overwhelmingly suffers from metabolic disorder, with a significant percentage of that undiagnosed. In other words- aren’t they very high?
I am not a doctor, but my low carb diet over the last three years has led my internal medicine doc to take me of my diabetes pill to see if I can maintain a HbA1c below 6 for me a 76 year male. I am 5’10, 31 waist and 148 lbs. No joint pains and never get the flus. The health care system concludes that a diabetic suffers from metabolic syndrome and LDL needs to be below 2 mmol/l and a statin is prescribed. I am on 5mg Crestor. LDL is 1.49/mmol/L
Why then do I keep discovering that this conclusion comes from studies using a population base that is typically on a high carb diet (the pyramid) This diet that includes fructose contributes to the glycation of LDL and this small LDL is likely more damaging to the arteries. Fluffy LDL, I read, actually heals arteries. But statins prevent this healing function and may trigger the onset of diabetes. In lay terms when you discover the fire fighters as the only ones at the scene of the fire, you could suspect they started the fire. What I need to know is whether the ratio of Triglycerides to HDL is a more reliable yet an imperfect predictor of the risk of heart disease over the next 10 years for me than LDL Thank you
“the status/permeability of the endothelium, the number of apoB containg particles, external facors like smoking, the presence of diabetes etc.”
Whole food bland based diet solves this problem…Nitric Oxide production and endothelial repair: see Dr. Caldwell Esselstyn ‘s work.
So much virtue signaling in these posts. We have the Low Carb High Animal Fat zealots who want to convince themselves that high ApoB is not a problem as long as your Trigs are low and HDL high and we have the Esselstyn nuts who believe his lie that plants can magically reverse clogged arteries. Then we have outcome based data from quality studies in humans confirmed by Mendelian randomization that high ApoB independent of ANY other risk factors (inflammation, particle size, HDL, trigs you name it) is causal in CVD. People with genetically crazy low ApoB have 0 heart disease. And low carb is awesome btw, provided you do it plant based or Mediterranean style. All the LC benefits without the strokes and heart attacks. Win win.
snarky! I like it! Hearing more and more docs that maintain up to date knowledge of the latest research say “all they care about is ApoB”. HDL, LDL, HDL/LDL ratio, triglycerides, etc all are meaningless except ApoB. Currently so few people are tested for ApoB; they are only guessing at the healthy range and “who” are getting tested??? Mostly people w problems.
I asked AI your question and got this answer if it is helpful: “I see a few points in that forum comment that are partially true, mixed with some common misconceptions about LDL, particle size, and statins.
Here’s a breakdown:
⸻
1. LDL-C of 1.49 mmol/L (~58 mg/dL)
• That’s already very low — most cardiology guidelines would consider that an optimal LDL-C for someone with diabetes or high cardiovascular risk.
• At that level, particle number (ApoB) is likely also low, but confirming with an ApoB test would be more accurate.
⸻
2. “Studies use a high-carb population, so results don’t apply to low-carb eaters”
• It’s true that most epidemiologic studies reflect a population eating higher carb diets.
• But LDL particle number (ApoB) predicts cardiovascular events across many dietary patterns — the harmful effect of high ApoB is consistent whether you’re low-carb, high-carb, or somewhere in between.
• A low-carb diet can shift LDL particles toward larger sizes, but if ApoB is high, risk remains.
⸻
3. “Small LDL is more damaging, large LDL heals arteries”
• Small, dense LDL is more strongly linked to atherogenesis than large, buoyant LDL — but this is largely because small LDL usually means you have more particles overall.
• Large LDL isn’t “healing” arteries; it’s just less atherogenic per particle. A high number of large LDL particles still drives plaque buildup.
• The claim that large LDL “heals arteries” isn’t supported by mainstream lipid research.
⸻
4. “Statins prevent this healing function and trigger diabetes”
• Statins can slightly raise blood sugar and tip some people into diabetes — but the effect is modest (about a 9% relative increase in diabetes incidence).
• Statins don’t block LDL from “healing” arteries; rather, they lower the number of LDL particles and reduce inflammation in the arterial wall.
⸻
5. TG/HDL ratio as a predictor
• TG/HDL ratio is a good proxy for insulin resistance and tends to correlate with LDL particle size.
• In someone with low TG and high HDL, small LDL is usually low — but ApoB is still the more precise predictor of atherosclerotic risk.
• TG/HDL ratio is imperfect because it doesn’t account for all LDL particle number variations.
⸻
6. For this individual
• With LDL-C ~58 mg/dL on 5 mg rosuvastatin, risk from LDL particles is probably already very low.
• If ApoB is also low (likely <65 mg/dL), then TG/HDL ratio adds little extra predictive value.
• The incremental benefit of staying on the statin might be modest — but it’s still protective for someone with diabetes history.
⸻
✅ Bottom line:
• ApoB is the gold standard for assessing LDL-related risk, not LDL particle size or TG/HDL ratio alone.
• Low-carb diets can improve particle size and insulin sensitivity, but they don’t make high ApoB harmless.
• This individual’s LDL-C is already very low, so their ApoB is likely already in the “low-risk” range — the debate for them is more about whether the statin adds enough extra protection to justify staying on it.
Agree that ApoB is the go to best test in diagnosis and management of lipids in patients with atherosclerosis and at risk patients who want to be more aggressive. The Bale-Doneen method preaches this from lesson one and has fantastic statistics on reduction of MACE and death and Alzheimer’s with their method. Drs. Bale and Doneen have provided multiple studies over the last 20 years stating what you have summarized above quite well. 20 YEARS of data on APOB being the real deal.
The world at large has gone wild with inappropriate hysteria over statins. All of us stop statins for side effects. At birth we have lipid levels so low you would guess the brain could not develop (and it does develop). These crazies on the internet preaching too low cholesterol numbers causing dementia (avoid high dose statins to avoid this probability). Follow the science and let’s put a Wonder Woman lasso on the TVs and computer monitors of the public so what we have learned is what patients trust.
BCBS of ALABAMA calls APO B experimental and there is no one on the planet who can hold them accountable for this erroneous misconception. We also need to change our DO/MD programs and testing platforms to adopt this APOB absolutely necessary change in practice. I’ve passed ABIM boards 3 times and I’m not sure they have adopted this “new” practice information.
It took us 20 years to stop radiating the babies of pregnant women so I guess sooner or later we will come around on this as well……
I agree! If Doc Sigurdsson and researchers know it’s a superior prediction to LDL, they should immediately switch to that test over LDL. I’m going to ask my doctor for it at my next annual exam. If he won’t administer it, I found a private lab that will do it. It’s not that expensive, and so important, everyone concerned about their heart health should get it from their doctor, or pay a private lab to do it. The lab I found will also do an apoA1 test. I just looked over notes I took from Docs Opinion in 2016, and even back then he said apoB is better than LDL. He also said in 2016 that apoB/apoA1 is a better marker of risk than lipids, lipoproteins and lipid ratios, and is more effective at predicting heart attack risk, than either the apoB or ApoA1 measure alone.