
Estimated reading time: 11 minutes
Loss of muscle mass, also called sarcopenia, is often considered a normal part of aging. Just like bone density decreases with age, loss of muscle mass and strength also occurs.
Loss of skeletal muscle mass may start as early as in our thirties and appears to continue for the rest of our lives.

Evidence suggests that muscle mass declines after 30 years of age at a rate of 3%–5% every ten years and that this decline accelerates after the age of 60 (1).
In the eighties, we may have lost about 50 percent of the muscle mass we managed to collect during our youth (2).
However, sarcopenia is not only about the loss of muscle mass. There is also loss of muscle strength and muscle function. The consequences may often be severe, particularly in the elderly.
Balance and gait often become affected. Hence, daily tasks such as rising from a chair unassisted or the ability to walk independently may become problematic, leading to loss of independence.
There is a decline in physical performance, a higher risk of disability, and reduced quality of life.
Studies show that sarcopenia is associated with frailty, risk of falling, and several adverse health outcomes among the elderly (3).
Why Does Age-Related Loss of Muscle Mass Occur?
There are several reasons behind age-related loss of muscle mass and strength.
Firstly, age-related molecular changes affecting muscles and motor neurons may play an important role (4).
Aging appears to result in an imbalance between muscle protein production and breakdown, leading to an overall loss of skeletal muscle (5).
Secondly, inflammation and hormonal changes appear to be involved.
Thirdly, environmental causes play a crucial role. The most important ones are reduced muscle activity and declines in nutritional intake.
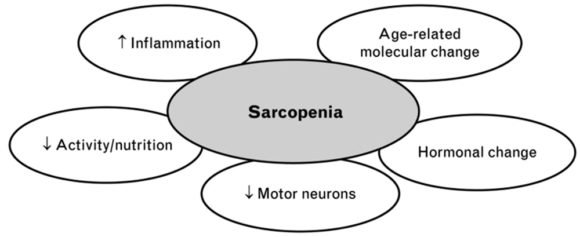
Physical inactivity is a strong risk factor for sarcopenia. Low physical activity and a sedentary lifestyle promote age-related muscle loss (5,6).
Furthermore, inadequate protein and calorie intake seem to play a critical role (7).
However, things are not always this simple because, in many individuals, age-related loss of muscle mass is accompanied by fat gain (8).
Hence, an excessive amount of fat tissue may contribute to loss of muscle mass and strength with aging (9). The term sarcopenic obesity has been used to describe this phenomenon.
Patients with diabetes appear to be at increased risk of sarcopenia (10).
Deficiency of micronutrients such as vitamin D, selenium, magnesium, and omega 3 fatty acids may also be important (11).
How Can Age-Related Muscle Mass Be Prevented?
Although regarded as a normal part of aging, sarcopenia development may be delayed and prevented to a certain degree.
Increased physical activity and adequate nutrition are the most powerful tools at our disposal for this purpose.
Although large-scale clinical trials are lacking, studies show that several measures may improve muscle strength and physical function. These may potentially slow the development of age-related loss of muscle mass.
The most substantial emphasis should focus on exercise and nutritional interventions.
The Role of Physical Exercise
There is no doubt that physical exercise increases muscle mass, reduces body fat, and improves muscle strength. Furthermore, physical endurance, immune and cardiovascular function are all improved.
Many studies show that muscular strength and strength training are associated with several health benefits and increased life expectancy (6,12).
Young people with low physical fitness are 3- to 6-fold more likely to develop diabetes, hypertension, and metabolic syndrome than individuals with high fitness (12).
Studies have shown that progressive resistance training counteracts muscle weakness and physical frailty (13).
Resistance training is probably the best type of exercise to prevent the loss of muscle mass and function.
Resistance training is any exercise that causes the muscles to contract against an external load or resistance. The external resistance can be your own bodyweight or any other object that causes the muscles to contract.
The resistance may dynamic, as in weightlifting or running, or static, as in activities like gymnastics and yoga (14).
No single type of exercise has been found to be effective in preventing age-related sarcopenia. Well-rounded exercise programs consisting of aerobic and resistance exercises are believed to be most effective (15).
The Role of Nutrition
Research shows that we often eat less and make different food choices as we age. The daily volume of foods and beverages tends to decline as a function of age.
Lower food intake among the elderly has been associated with lower intakes of calcium, iron, zinc, B vitamins, and vitamin E (16).
It is still unclear what impact these dietary changes may have on the health of the elderly individual.
However, modification of dietary habits may be an important tool to prevent the decline in muscle mass and function that occurs with aging.
Studies of frailty among the elderly show that low nutrient intake is a risk factor. This is especially true for diets low in protein (17).
One study suggested that promoting the intake of animal protein and monounsaturated fatty acids (MUFAs) might reduce frailty (18).
Another study showed that the intake of five servings of fruits and vegetables a day is associated with less frailty (19).
Similarly, a Mediterranean diet is associated with a decreased risk of frailty (20)
Fish consumption has a protective effect on skeletal muscle and maintains good muscle performance, preventing sarcopenia (21).
Fish protein is of high biological value. Fish also provides essential micronutrients such as omega 3, magnesium, and Vitamin E and D.
Proteins, Peptides and Amino Acids
Proteins are a class of organic compounds that are vital to every living cell.
Proteins are composed of one or more long chains of amino acids.
Peptides are shorter chains of amino acids. A peptide often consists of only two or three amino acids.
According to the current definition, peptides consist of less than 50 amino acids, whereas proteins are made up of 50 or more amino acids.
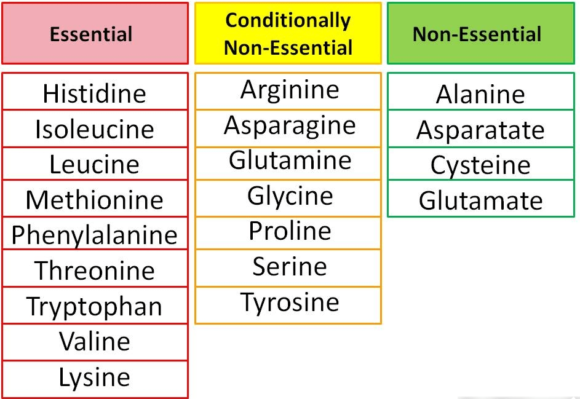
Although approximately 500 amino acids have been identified in nature, only 20 make up the human body’s proteins (22). These 20 amino acids are the building blocks for all the proteins in the body.
Amino acids are organic compounds composed of nitrogen, carbon, hydrogen, and oxygen, along with a side-chain group.
Amino acids are classified into two types, essential or non-essential.
The non-essential amino acids can be synthesized by the body whereas the essential ones cannot. Hence, essential amino acids have to be present in our diet.
Some amino acids are considered conditionally non-essential, meaning that they are usually not essential, except in times of illness and stress (23).
Proteins and Sarcopenia
Amino acids are needed for the synthesis of muscle protein. Dietary protein is our primary source of amino acids.
Low protein consumption is associated with loss of muscle mass in the elderly (24).
Vegetable proteins tend to be deficient in one or more essential amino acids, whereas protein from animal sources is not. Hence, animal-derived protein may provide a higher and broader biological value.
Recent studies suggest that protein supplementation can help to prevent age-related loss of muscle mass (25, 26).
However, there is currently no basis for recommending high protein/high meat intake above the recommended dietary allowance for healthy adults.
High-protein/high-meat diets may be associated with several health risks and may impose a metabolic burden on the bones, kidneys, and liver (27).
Muscle Protein Turnover and Sarcopenia
Proteins are a key component of skeletal muscle.
Muscle mass is dependent on the balance between the rate at which muscle proteins are synthesized and degraded.
All essential and non-essential amino acids have to be present in adequate amounts for normal muscle protein production to take place (28).
During sarcopenia, the rate of muscle protein breakdown exceeds muscle protein synthesis. This will inevitably lead to loss of muscle mass over time.
Several factors may influence whether muscle protein breakdown exceeds muscle protein synthesis or not.
Importantly, muscle protein synthesis appears to increase following protein intake (29).
Essential amino acids are primarily responsible for stimulating muscle protein synthesis in the elderly (30).
Branched-Chain Amino Acids
Three of the essential amino acids, leucine, isoleucine, and valine, are termed branch chain amino acids.
Branched-chain amino acids appear to play a key role in stimulating muscle protein synthesis (31). This is particularly true for the amino acid leucine.
Interestingly, a multi-million dollar industry has evolved around the concept that nutritional supplements of branched-chain amino acids alone will drive muscle synthesis.
However, evidence suggests that the availability of other essential amino acids is of key importance as well. Hence, the intake of branched-chain amino acids alone may not be enough to promote muscle synthesis (28).
Whey Protein and Sarcopenia
Whey protein is found in dairy products. It is a liquid material leftover from milk during cheese production and contains substantial amounts of essential amino acids.
Whey protein is typically used in the form of a powder. There are three main types; concentrate (WPC), isolate (WPI), and hydrolysate (WPH) (32).
A randomized study showed that vitamin D and leucine-enriched whey protein nutritional supplement resulted in improvements in muscle mass and lower-extremity function among sarcopenic older adults.
The authors of the paper suggested that the study shows proof-of-principle that specific nutritional supplementation alone might benefit frail elderly patients, especially those who are unable to exercise (33).
Evidence suggests that daily dietary supplementation of 35 g of whey is likely to improve some markers of sarcopenia (34).

The Potential Role of Role of Fish Derived Protein
Fish provides an important dietary source of protein for humans.
However, the fishing industry generates more than 60 percent of its product as rest or waste. These products include skin, head, viscera, liver, frames, bones, and roes (35).
Interestingly, these unused byproducts may represent high-quality sources of protein and other nutrients.
By using a special technique called enzymatic hydrolysis, vital proteins may be recovered from waste products that would typically be disposed of (36). These products are called fish protein hydrolysates (37).
Fish protein hydrolysates mainly provide short peptides that are composed of two or three amino acids. Such peptides are absorbed more readily than free amino acids and much more rapidly than intact protein.
Studies strongly suggest that ingestion of protein hydrolysates provides a rapid increase in amino acids in the circulation (38).
Faster absorption may have several positive clinical implications. For example, it could be an important issue for muscle health and muscle recovery in athletes.
Studies on the effects of fish-derived protein hydrolysates on age-related loss of muscle mass and muscle function are underway (39).
Micronutrients and Sarcopenia
Vitamin D
Elderly individuals with low serum concentrations of Vitamin D are at increased risk of age-related loss of muscle mass (40).
A decline in serum Vitamin D concentration with advanced age also results in reduced bone density, leading to a higher risk of falling and bone fractures.
Studies have shown that Vitamin D supplementations improve muscle strength. The effect appears to be most pronounced among individuals with low serum concentration of Vitamin D, common among the elderly (41).
Although there are some promising data regarding the role of vitamin D and sarcopenia, it is unclear how the dose and length of treatment impact vitamin D’s efficacy in improving muscle mass or function (42).
Vitamin C
One of the proposed underlying mechanisms causing sarcopenia is oxidative stress.
Hence, Vitamin C, as an anti-oxidant, might play a role.
Recently, a relatively large epidemiological survey showed low blood levels of vitamin C were associated with an increased risk of sarcopenia among the elderly (27). Data from the same study showed an association between C-vitamin intake and muscle mass.
However, previous studies have shown mixed results when it comes to vitamin C intake and muscle strength.
Vitamin B12
Vitamin B12 deficiency is common in older adults.
One study found that Vitamin B12 deficiency may be related to sarcopenia among the elderly (28).
Another study found that serum levels of vitamin B12 were 15% lower among sarcopenic individuals compared to healthy controls (29).
So, ruling out and treating B12 deficiency is essential to prevent and treat sarcopenia..
Minerals
Minerals may help to prevent and/or treat sarcopenia.
Magnesium, selenium, and calcium in particular seem to be most promising.
However, the association of mineral supplements with sarcopenia is mainly based on observational studies. Hence, randomized controlled trials are needed to elucidate the potential benefits of minerals for healthy muscle aging.
The Take-Home Message
Age-related loss of muscle mass (sarcopenia)may start as early as in our thirties and appears to continue for the rest of our lives.
There is also a loss of muscle strength and muscle function. The consequences may often be severe, particularly in the elderly.
Increased physical activity and adequate nutrition are the most powerful tools at our disposal to delay age-related loss of muscle mass.
Well-rounded exercise programs consisting of aerobic and resistance exercises are believed to be most effective
Modification of dietary habits may be an important tool to prevent the decline in muscle mass and function that occurs with aging.
Adequate protein intake is of key importance. Animal-derived protein may provide a higher and broader biological value than vegetable protein.
Fish consumption is recommended and fruits and vegetables should be consumed regularly.
Nutritional supplements containing essential amino acids may be helpful. This is particularly true for whey protein.
Fish-derived protein hydrolysates also appear promising.
Adequate intake of vitamin D is essential.
“Vitamin C, as an oxidant” shouldn’t this read “as an anti-oxidant”?
Thanks Ian.
Of course you are absolutely correct.
Thanks for reading so thoroughly.
I’ve corrected the mistake.
Axel
Typically, researchers don’t think to reduce linoleic acid and arachidonic acid intake to attenuate inflammation.[1] It’s all about adding omega-3s.[2] Excerpt: “Because arachidonic acid (AA) competes with EPA and DHA as well as with LA, ALA and oleic acid for incorporation in membrane lipids at the same positions, all these fatty acids are important for controlling the AA concentration in membrane lipids, which in turn determines how much AA can be liberated and become available for prostaglandin biosynthesis following phospholipase activation. Thus, the best strategy for dampening prostanoid overproduction in disease situations would be to reduce the intake of AA, or reduce the intake of AA at the same time as the total intake of competing fatty acids (including oleic acid) is enhanced, rather than enhancing intakes of EPA and DHA only.[3]
1. https://www.frontiersin.org/articles/10.3389/fphys.2017.01045/full
2. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6583677/
3. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2875212/
4.