Recent scientific evidence shows that the blood concentration of lipoprotein(a) (Lp(a)) is an important marker for the risk of developing heart disease. Nonetheless, Lp(a) measurements are not widely available and are seldom used in routine clinical practice.
A traditional lipid panel does not include measurements of lipoprotein(a)
Lately, measuring the concentration or number of lipoprotein particles has been found to be useful to assess risk. Examples of such measurements are measurements of LDL particle number (LDL-P), apolipoprotein B and Lp(a).
It has been known for some time that Lp(a) is a decisive risk factor for developing coronary heart disease and calcific narrowing of the aortic valve (aortic valve stenosis). However, the lack of clinical trial data has caused it to be largely ignored by the medical community. This is mainly due to the absence of lifestyle measures or therapies that may lower blood levels of Lp(a).
Blood levels of Lp(a) are genetically determined, meaning that environmental factors have a limited influence on the blood levels of the substance.
What Is Lipoprotein(a)?
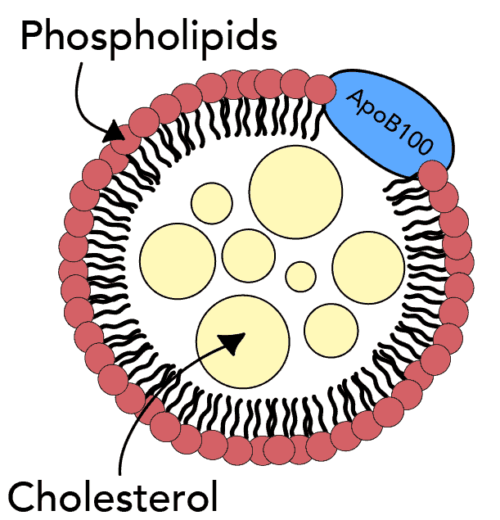
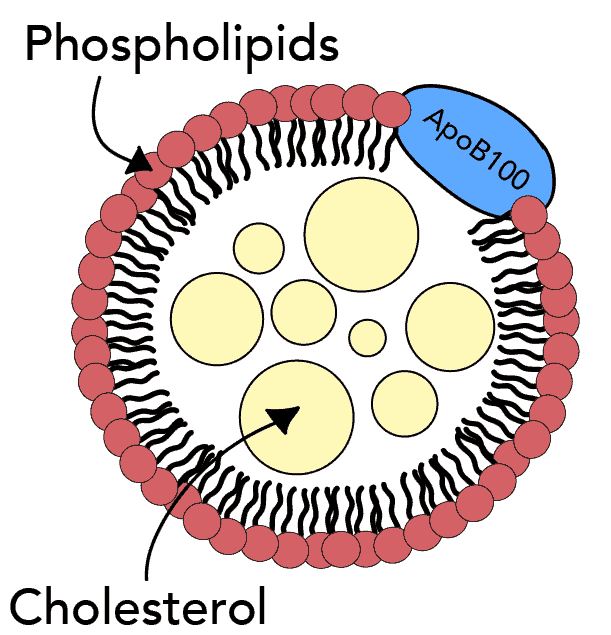
Lipoproteins are particles that transport cholesterol and triglycerides in the bloodstream. They are composed of proteins (apolipoproteins), phospholipids, triglycerides, and cholesterol.
The lipoproteins vary in the major lipoprotein present and the relative contents of the different lipid components.
Lipoproteins that promote atherosclerosis (the leading underlying cause of heart disease) are termed atherogenic. ApoB is an essential component of all atherogenic lipoproteins.
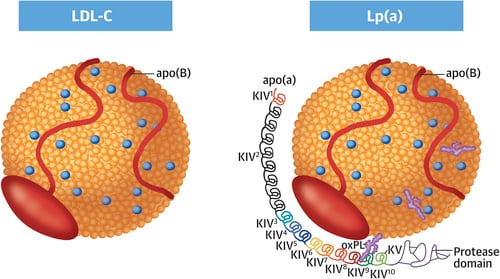
Lp(a)consists of an LDL-like core lipoprotein molecule but differs from other lipoproteins as it contains a unique apolipoprotein(a) or apo(a)
How Does an Excess of Lipoprotein(a) Cause Heart Disease?
There are several mechanisms by which Lp(a) may cause heart disease.
Firstly, like all other Apo B containing lipoproteins, Lp(a) may enter the arterial wall and promote inflammatory reactions, subsequently leading to atherosclerosis (3).
Secondly, Lp(a) is an important carrier of oxidized phospholipids (OxPLs) (4).
Blood levels of OxPLs have been previously demonstrated to be strongly associated with atherosclerotic cardiovascular disease (5). Furthermore, OxPLs seem to be associated with an increased risk of developing calcified aortic valve stenosis (6).
Thirdly, the apolioprotein (a) component of Lp(a) resembles plasminogen, an important enzyme participating in the dissolution of blood clots. Therefore, it has been suggested that high levels of Lp(a) may inhibit the natural role of plasminogen and thereby increase the risk of blood clots (7).
Lipoprotein(a) and Coronary Heart Disease
Several studies have shown that Lp(a) is a significant risk factor for developing coronary heart disease.
In a summary of 36 cohort studies, Lp(a) levels were found to be associated with increased risk of coronary heart disease and stroke (8).
In the Copenhagen City Heart Study, elevated Lp(a) levels were associated with a 1.9- and 2.6-fold increased risk of myocardial infarction (heart attack) over a 16-year follow-up period (9).
Mendelian randomization studies have provided strong evidence for a direct causative role of Lp(a) in the development of coronary heart disease (10, 11, 12).
A recently published case-control study predicted that pharmacologic reduction of Lp(a) in individuals with the highest concentration would substantially decrease the risk of cardiovascular disease (13).
Lipoprotein(a) and Aortic Valve Stenosis
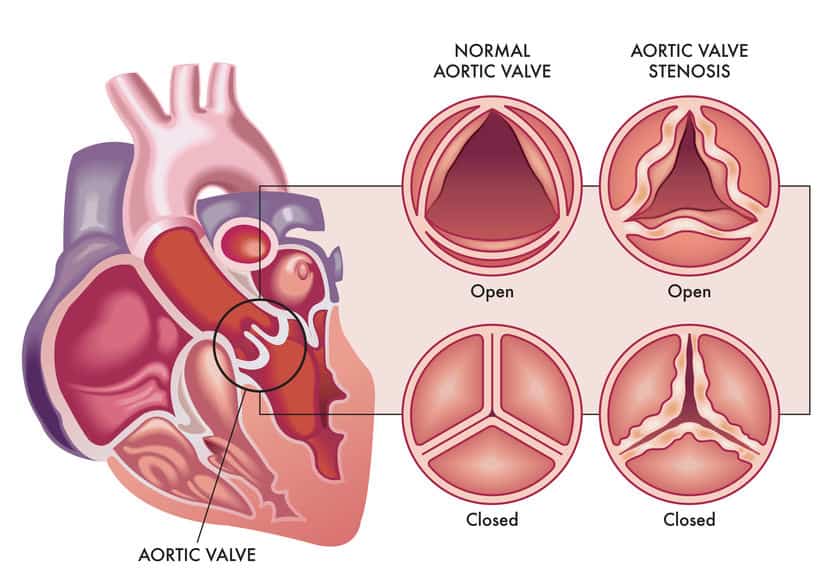
Aortic valve abnormalities are pretty frequent in older people. A thickening or calcification of the aortic valve or calcification, without significant obstruction, is found in 26 percent of people older than 65 years (14).
In some people, the aortic valve’s leaflets may become stiff, leading to a narrowing of the aortic valve opening. If severe, this may obstruct blood flow from the left ventricle; a condition called aortic valve stenosis.
Clinical studies demonstrate a significant association between Lp(a) levels and aortic valve stenosis.
Furthermore, genome-wide and Mendelian randomization studies suggest that high Lp(a) levels play a causative role in developing the disorder (4).
What Is the Normal Range For Blood Levels of Lipoprotein(a)?
Here’s how Lp(a) levels are looked at in terms of risk:
Desirable: < 14 mg/dL (< 35 nmol/l)
Borderline risk: 14 – 30 mg/dL (35 – 75 nmol/l)
High risk: 31 – 50 mg/dL (75 – 125 nmol/l)
Very high risk: > 50 mg/dL (> 125 nmol/l)
How Can Lipoprotein(a) Be Modulated?
Lp(a) levels are primarily genetically determined. Nonetheless, lifestyle factors may also play a role.
Studies on the effect of diet on Lp(a) levels are limited. However, low-fat diets, in particular, seem to result in a small but significant increase in Lp(a)(15,16)
Interestingly, a low-fat, high-carbohydrate diet may increase Lp(a) levels compared to a high-fat, low-carbohydrate diet (16).
The data on the effect of statin drugs on Lp(a)levels are conflicting.
For example, one study showed that statins significantly increase plasma Lp(a) levels (17). However, the same study suggested that statins lowered non-HDL cholesterol substantially and reduced overall cardiovascular risk.
Niacin decreases Lp(a) levels by approximately 20%-30% (18).
PCSK9 inhibitors lower Lp(a) by approximately 20%-30% (4).
Recently, Lp(a)-specific lowering medications have become available. Major ongoing clinical trials are investigating the clinical efficacy of these agents in patients with elevated Lp(a) levels.
The HORIZON phase III trial is investigating the benefit of Lp(a)-lowering with an antisense oligonucleotide (ASO), TQJ230, compared to placebo, on major cardiovascular events, in patients with established cardiovascular disease (19).
The Take-Home Message
Lipoprotein(a) is a strong risk factor for developing coronary heart disease and calcific narrowing of the aortic valve (aortic valve stenosis).
Mendelian randomization studies have provided strong evidence for a direct causative role of Lipoprotein(a) in developing these disorders.
Lipoprotein(a) levels are primarily genetically determined. Nonetheless, lifestyle factors may also play a role.
High-fat, low-carbohydrate diets lower lipoprotein(a) more effectively than low-fat diets.
Major ongoing clinical trials are currently investigating the clinical efficacy of specific lipoprotein(a)-lowering agents in patients with elevated lipoprotein(a) levels.
Apolipoprotein B (ApoB) is a protein that plays an important role in the development of heart disease. Elevated blood levels of ApoB indicate an increased risk.
Actually, ApoB may be a stronger predictor of risk than commonly used lipid markers such as LDL-cholesterol (1).
ApoB is an important component of lipoproteins that participate in the formation of atherosclerosis.
To help you understand the role of ApoB, I will start by briefly explaining the role of lipoproteins in atherosclerosis. I will then discuss the apolipoproteins and their different classes. Finally, I will explain the role of ApoB and how it can be used to assess the risk of heart disease.
Atherosclerosis
Atherosclerosis may be described as chronic inflammation of the arterial wall. It is caused by a complex interplay between lipoproteins, white blood cells (macrophages), the immune system, and the arterial wall’s normal elements.
Atherosclerosis is initiated when an apoB-containing lipoprotein particle is caught in the vessel wall. This leads to an inflammatory cascade, resulting in the progression of atherosclerosis.
Atherosclerosis leads to the formation of plaques within the walls of the arteries. These plaques may subsequently cause blockages and limit blood flow to tissues and organs such as the heart and the brain.
A rupture of an atherosclerotic plaque (plaque rupture) may lead to thrombosis (blood clotting), causing an artery’s abrupt occlusion (blockage). If this occurs in a coronary artery, it may cause an acute myocardial infarction (acute heart attack).
Cholesterol and Lipoproteins
Although cholesterol is an essential substance for most cells in our body, elevated blood levels may play a role in the initiation and progression of atherosclerosis.
In animal models, atherosclerosis will not occur in the absence of greatly elevated levels of plasma cholesterol. High blood levels of cholesterol also appear to be an important contributor to atherosclerosis in humans.
However, the role of cholesterol is most often oversimplified. Many individuals with high blood cholesterol never develop heart disease, and many patients with heart disease don’t have high cholesterol levels.
In fact, cholesterol’s role in heart disease appears to be determined by the lipoproteins that carry the cholesterol in the bloodstream rather than the cholesterol itself.
Let me explain.
Because fats are insoluble in water, cholesterol can not be transported in blood on its own.
The body’s solution to this problem is to bind fats to proteins that function as transport vehicles carrying different types of fats such as cholesterol, triglycerides, and phospholipids. These combinations of fats and protein are termed lipoproteins
It is important to emphasize that it is the lipoproteins (not the cholesterol) that interact with the arterial wall and initiate the cascade of events that leads to atherosclerosis (2).
Cholesterol is only one of many components of lipoproteins. Therefore, measurements of total cholesterol provide little information about the amount and types lipoproteins particles in the circulation.
Lately, the role of another lipoprotein, called lipoprotein(a) or Lp(a), has been highlighted (3).
A standard lipid profile will tell us how much cholesterol is being carried by the different lipoproteins. Hence, the level of LDL-cholesterol and HDL-cholesterol will tell us how much cholesterol is found within LDL and HDL particles, respectively.
Scientific data tells us that there is a strong correlation between LDL-cholesterol and heart disease risk, although this has been debated by some investigators (3, 4).
However, measurements of the number of LDL-particles appear more predictive of risk than the cholesterol mass within these particles (represented by LDL-cholesterol) (5,6).
Apolipoproteins
Lipoproteins are comprised of apolipoproteins, phospholipids, triglycerides, and cholesterol. However, the lipoproteins vary in the major proteins present and their lipid components differ.
Different lipoproteins contain different types of apolipoproteins. The type of apolipoprotein present determines the structure and function of the lipoprotein.
There are several classes of apolipoproteins and many subclasses (7).
ApoA5 is a marker of increased triglyceride concentrations and a risk factor for heart disease in some populations (9).
ApoD has antioxidant and anti-inflammatory activity. It may play a role in diseases of the nervous system and the aging process (10).
ApoE has several subclasses. Human ApoE exists as three common isoforms, ApoE2, ApoE3, and ApoE4 (11).
ApoE4 is a major genetic risk factor for late-onset Alzheimer’s disease (12).
The type of apolipoprotein present determines the structure and function of the lipoprotein. ApoB100 is an important component of lipoproteins that promote atherosclerosis.
Apolipoprotein B
Retention of ApoB containing lipoprotein particles within the arterial wall is an essential part of the early atherosclerotic process.
Lipoproteins that promote atherosclerosis are termed atherogenic. ApoB is an important component of all atherogenic lipoproteins.
Human ApoB has two main forms, apoB48 and apoB100. ApoB48 is synthesized mainly by the small intestine, and ApoB 100 ,is synthesized by the liver (13).
From the viewpoint of atherosclerosis and cardiovascular risk, apoB100 is the important one.
ApoB 48 is primarily found in chylomicrons whereas ApoB 100 is found in chylomicrons, LDL, very-low-density lipoprotein (VLDL), intermediate-density lipoprotein (IDL), and Lp(a) particles.
Atherogenic lipoproteins such as LDL, VLDL, and Lp(a) all contain one ApoB molecule per particle. Hence, measurements of ApoB reflect the number of atherogenic particles.
On the other hand, HDL does not contain ApoB and is not atherogenic. In fact, HDL appears to play a protective role, and high numbers of HDL particles are associated with less risk of heart disease (2).
As mentioned before, ApoA-1 is the principal apolipoprotein on the HDL paritcle.
Thus, the ApoB/ApoA-1 ratio represents a measure of the balance between particles that promote and protect from athersclerosis.
The ApoB/ApoA1 ratio may be more effective at predicting heart attack risk than either the apoB or apoA1 measure alone (14).
Usually, 85-90 percent of apoB is found in LDL particles. Thus, apoB reflects LDL particle number, similar to LDL-P.
Evidence suggests that apoB is a better tool to predict cardiovascular risk than LDL-cholesterol and non-HDL-cholesterol (15).
Furthermore, apoB may be elevated despite normal or low levels of LDL-cholesterol (16).
ApoB also appears to predict risk when LDL-cholesterol has been lowered by statin therapy.
Normal Range For Apolipoprotein B
Although measurements of apoB are not widely available, the assay has been standardized and does not require a fasting sample.
The normal range for apoB is 40-125 mg/dL.
ApoB levels are higher in men than women and tend to increase with age.
Here is how apoB levels are looked at in terms of risk of heart disease:
Less than 130 mg/dL (1.3 g/L)is considered desirable in individuals without risk factors.
Less than 110 mg/dL (1.1 g/L) is considered desirable in low or intermediate-risk individuals.
Less than 90 mg/dL (0.9 g/L) is desirable in high-risk individuals, such as those with heart disease or diabetes.
How to Lower Apolipoprotein B
Many experts will recommend the same general measures to lower apoB as they do for lowering LDL-cholesterol. Hence, eating less saturated fat and cholesterol from meat and dairy products is often regarded as a first step. Furthermore, increased consumption of vegetables, fiber, and mono-and polyunsaturated (omega-3) fatty acids is recommended.
However, some dietary interventions may affect LDL-cholesterol and apoB differently. For example, some studies have indicated that carbohydrate restriction may lower apoB, independent of whether the intake of saturated fat is high or low (17).
Patients with high levels of triglycerides and low HDL-cholesterol may have high apoB levels despite normal or low LDL-cholesterol. These patients may derive most benefit from low-carbohydrate diets (18).
Loss of muscle mass, also called sarcopenia, is often considered a normal part of aging. Just like bone density decreases with age, loss of muscle mass and strength also occurs.
Loss of skeletal muscle mass may start as early as in our thirties and appears to continue for the rest of our lives.
Evidence suggests that muscle mass declines after 30 years of age at a rate of 3%–5% every ten years and that this decline accelerates after the age of 60 (1).
In the eighties, we may have lost about 50 percent of the muscle mass we managed to collect during our youth (2).
However, sarcopenia is not only about the loss of muscle mass. There is also loss of muscle strength and muscle function. The consequences may often be severe, particularly in the elderly.
Balance and gait often become affected. Hence, daily tasks such as rising from a chair unassisted or the ability to walk independently may become problematic, leading to loss of independence.
There is a decline in physical performance, a higher risk of disability, and reduced quality of life.
Studies show that sarcopenia is associated with frailty, risk of falling, and several adverse health outcomes among the elderly (3).
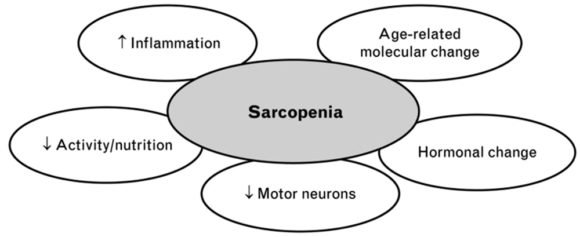
Why Does Age-Related Loss of Muscle Mass Occur?
There are several reasons behind age-related loss of muscle mass and strength.
Firstly, age-related molecular changes affecting muscles and motor neurons may play an important role (4).
Aging appears to result in an imbalance between muscle protein production and breakdown, leading to an overall loss of skeletal muscle (5).
Secondly, inflammation and hormonal changes appear to be involved.
Thirdly, environmental causes play a crucial role. The most important ones are reduced muscle activity and declines in nutritional intake.
Multifactorial causes of sarcopenia. https://doi.org/10.4081/gc.2019.8033
Physical inactivity is a strong risk factor for sarcopenia. Low physical activity and a sedentary lifestyle promote age-related muscle loss (5,6).
Furthermore, inadequate protein and calorie intake seem to play a critical role (7).
However, things are not always this simple because, in many individuals, age-related loss of muscle mass is accompanied by fat gain (8).
Hence, an excessive amount of fat tissue may contribute to loss of muscle mass and strength with aging (9). The term sarcopenic obesity has been used to describe this phenomenon.
Patients with diabetes appear to be at increased risk of sarcopenia (10).
Deficiency of micronutrients such as vitamin D, selenium, magnesium, and omega 3 fatty acids may also be important (11).
How Can Age-Related Muscle Mass Be Prevented?
Although regarded as a normal part of aging, sarcopenia development may be delayed and prevented to a certain degree.
Increased physical activity and adequate nutrition are the most powerful tools at our disposal for this purpose.
Although large-scale clinical trials are lacking, studies show that several measures may improve muscle strength and physical function. These may potentially slow the development of age-related loss of muscle mass.
The most substantial emphasis should focus on exercise and nutritional interventions.
The Role of Physical Exercise
There is no doubt that physical exercise increases muscle mass, reduces body fat, and improves muscle strength. Furthermore, physical endurance, immune and cardiovascular function are all improved.
Many studies show that muscular strength and strength training are associated with several health benefits and increased life expectancy (6,12).
Young people with low physical fitness are 3- to 6-fold more likely to develop diabetes, hypertension, and metabolic syndrome than individuals with high fitness (12).
Studies have shown that progressive resistance training counteracts muscle weakness and physical frailty (13).
Resistance training is probably the best type of exercise to prevent the loss of muscle mass and function.
Resistance training is any exercise that causes the muscles to contract against an external load or resistance. The external resistance can be your own bodyweight or any other object that causes the muscles to contract.
The resistance may dynamic, as in weightlifting or running, or static, as in activities like gymnastics and yoga (14).
No single type of exercise has been found to be effective in preventing age-related sarcopenia. Well-rounded exercise programs consisting of aerobic and resistance exercises are believed to be most effective (15).
The Role of Nutrition
Research shows that we often eat less and make different food choices as we age. The daily volume of foods and beverages tends to decline as a function of age.
Lower food intake among the elderly has been associated with lower intakes of calcium, iron, zinc, B vitamins, and vitamin E (16).
It is still unclear what impact these dietary changes may have on the health of the elderly individual.
However, modification of dietary habits may be an important tool to prevent the decline in muscle mass and function that occurs with aging.
Studies of frailty among the elderly show that low nutrient intake is a risk factor. This is especially true for diets low in protein (17).
One study suggested that promoting the intake of animal protein and monounsaturated fatty acids (MUFAs) might reduce frailty (18).
Another study showed that the intake of five servings of fruits and vegetables a day is associated with less frailty (19).
Similarly, a Mediterranean diet is associated with a decreased risk of frailty (20)
Fish consumption has a protective effect on skeletal muscle and maintains good muscle performance, preventing sarcopenia (21).
Fish protein is of high biological value. Fish also provides essential micronutrients such as omega 3, magnesium, and Vitamin E and D.
Proteins, Peptides and Amino Acids
Proteins are a class of organic compounds that are vital to every living cell.
Proteins are composed of one or more long chains of amino acids.
Peptides are shorter chains of amino acids. A peptide often consists of only two or three amino acids.
According to the current definition, peptides consist of less than 50 amino acids, whereas proteins are made up of 50 or more amino acids.
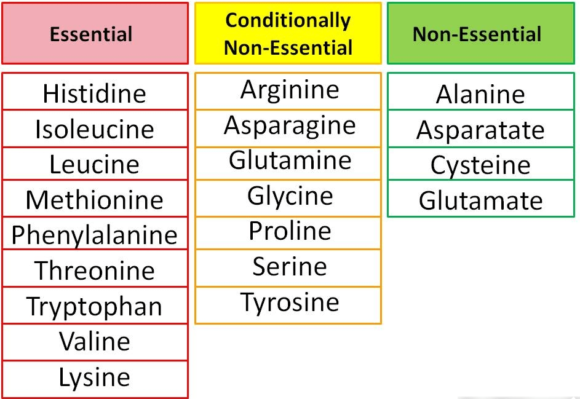
Although approximately 500 amino acids have been identified in nature, only 20 make up the human body’s proteins (22). These 20 amino acids are the building blocks for all the proteins in the body.
Amino acids are organic compounds composed of nitrogen, carbon, hydrogen, and oxygen, along with a side-chain group.
Amino acids are classified into two types, essential or non-essential.
The non-essential amino acids can be synthesized by the body whereas the essential ones cannot. Hence, essential amino acids have to be present in our diet.
Some amino acids are considered conditionally non-essential, meaning that they are usually not essential, except in times of illness and stress (23).
Amino acids are classified into essential, conditionally non- essential, and non-essential. Essential amino acids can not be produced by the body and have to be present in our diet.
Proteins and Sarcopenia
Amino acids are needed for the synthesis of muscle protein. Dietary protein is our primary source of amino acids.
Low protein consumption is associated with loss of muscle mass in the elderly (24).
Vegetable proteins tend to be deficient in one or more essential amino acids, whereas protein from animal sources is not. Hence, animal-derived protein may provide a higher and broader biological value.
Recent studies suggest that protein supplementation can help to prevent age-related loss of muscle mass (25, 26).
However, there is currently no basis for recommending high protein/high meat intake above the recommended dietary allowance for healthy adults.
High-protein/high-meat diets may be associated with several health risks and may impose a metabolic burden on the bones, kidneys, and liver (27).
Muscle Protein Turnover and Sarcopenia
Proteins are a key component of skeletal muscle.
Muscle mass is dependent on the balance between the rate at which muscle proteins are synthesized and degraded.
All essential and non-essential amino acids have to be present in adequate amounts for normal muscle protein production to take place (28).
During sarcopenia, the rate of muscle protein breakdown exceeds muscle protein synthesis. This will inevitably lead to loss of muscle mass over time.
Several factors may influence whether muscle protein breakdown exceeds muscle protein synthesis or not.
Importantly, muscle protein synthesis appears to increase following protein intake (29).
Essential amino acids are primarily responsible for stimulating muscle protein synthesis in the elderly (30).
Branched-Chain Amino Acids
Three of the essential amino acids, leucine, isoleucine, and valine, are termed branch chain amino acids.
Branched-chain amino acids appear to play a key role in stimulating muscle protein synthesis (31). This is particularly true for the amino acid leucine.
Interestingly, a multi-million dollar industry has evolved around the concept that nutritional supplements of branched-chain amino acids alone will drive muscle synthesis.
However, evidence suggests that the availability of other essential amino acids is of key importance as well. Hence, the intake of branched-chain amino acids alone may not be enough to promote muscle synthesis (28).
Whey Protein and Sarcopenia
Whey protein is found in dairy products. It is a liquid material leftover from milk during cheese production and contains substantial amounts of essential amino acids.
Whey protein is typically used in the form of a powder. There are three main types; concentrate (WPC), isolate (WPI), and hydrolysate (WPH) (32).
A randomized study showed that vitamin D and leucine-enriched whey protein nutritional supplement resulted in improvements in muscle mass and lower-extremity function among sarcopenic older adults.
The authors of the paper suggested that the study shows proof-of-principle that specific nutritional supplementation alone might benefit frail elderly patients, especially those who are unable to exercise (33).
Evidence suggests that daily dietary supplementation of 35 g of whey is likely to improve some markers of sarcopenia (34).
The Potential Role of Role of Fish Derived Protein
Fish provides an important dietary source of protein for humans.
However, the fishing industry generates more than 60 percent of its product as rest or waste. These products include skin, head, viscera, liver, frames, bones, and roes (35).
Interestingly, these unused byproducts may represent high-quality sources of protein and other nutrients.
By using a special technique called enzymatic hydrolysis, vital proteins may be recovered from waste products that would typically be disposed of (36). These products are called fish protein hydrolysates (37).
Fish protein hydrolysates mainly provide short peptides that are composed of two or three amino acids. Such peptides are absorbed more readily than free amino acids and much more rapidly than intact protein.
Studies strongly suggest that ingestion of protein hydrolysates provides a rapid increase in amino acids in the circulation (38).
Faster absorption may have several positive clinical implications. For example, it could be an important issue for muscle health and muscle recovery in athletes.
Studies on the effects of fish-derived protein hydrolysates on age-related loss of muscle mass and muscle function are underway (39).
Micronutrients and Sarcopenia
Vitamin D
Elderly individuals with low serum concentrations of Vitamin D are at increased risk of age-related loss of muscle mass (40).
A decline in serum Vitamin D concentration with advanced age also results in reduced bone density, leading to a higher risk of falling and bone fractures.
Studies have shown that Vitamin D supplementations improve muscle strength. The effect appears to be most pronounced among individuals with low serum concentration of Vitamin D, common among the elderly (41).
Although there are some promising data regarding the role of vitamin D and sarcopenia, it is unclear how the dose and length of treatment impact vitamin D’s efficacy in improving muscle mass or function (42).
Vitamin C
One of the proposed underlying mechanisms causing sarcopenia is oxidative stress.
Hence, Vitamin C, as an anti-oxidant, might play a role.
Recently, a relatively large epidemiological survey showed low blood levels of vitamin C were associated with an increased risk of sarcopenia among the elderly (27). Data from the same study showed an association between C-vitamin intake and muscle mass.
However, previous studies have shown mixed results when it comes to vitamin C intake and muscle strength.
Vitamin B12
Vitamin B12 deficiency is common in older adults.
One study found that Vitamin B12 deficiency may be related to sarcopenia among the elderly (28).
Another study found that serum levels of vitamin B12 were 15% lower among sarcopenic individuals compared to healthy controls (29).
So, ruling out and treating B12 deficiency is essential to prevent and treat sarcopenia..
Minerals
Minerals may help to prevent and/or treat sarcopenia.
Magnesium, selenium, and calcium in particular seem to be most promising.
However, the association of mineral supplements with sarcopenia is mainly based on observational studies. Hence, randomized controlled trials are needed to elucidate the potential benefits of minerals for healthy muscle aging.
The Take-Home Message
Age-related loss of muscle mass (sarcopenia)may start as early as in our thirties and appears to continue for the rest of our lives.
There is also a loss of muscle strength and muscle function. The consequences may often be severe, particularly in the elderly.
Increased physical activity and adequate nutrition are the most powerful tools at our disposal to delay age-related loss of muscle mass.
Well-rounded exercise programs consisting of aerobic and resistance exercises are believed to be most effective
Modification of dietary habits may be an important tool to prevent the decline in muscle mass and function that occurs with aging.
Adequate protein intake is of key importance. Animal-derived protein may provide a higher and broader biological value than vegetable protein.
Fish consumption is recommended and fruits and vegetables should be consumed regularly.
Nutritional supplements containing essential amino acids may be helpful. This is particularly true for whey protein.
Fish-derived protein hydrolysates also appear promising.
The death rate from coronary artery disease (CAD) has declined considerably over the last three decades. This is mainly due to better control of risk factors and advances in therapy.
However, the prevalence of CAD remains high due to the aging of the population and better survival of those affected.
The current epidemic of obesity and type 2 diabetes will likely escalate the problem further.
Atherosclerosis, the underlying cause of CAD, is characterized by an accumulation of lipids, white blood cells, and cell debris in the inner layers of the arterial wall. The immune system is involved in the process, and inflammation appears to play a critical role (1).
Atherosclerosis can affect all arteries in the body but seems to have a high affinity for the coronary arteries.
Atherosclerotic lesions or plaques may protrude into the lumen of the coronary arteries, causing blockages that may limit blood flow to the heart muscle.
Additionally, rupture of an atherosclerotic plaque may cause thrombosis (blood clotting), completely blocking blood flow in a coronary artery. The result may be an acute heart attack.
The Role of Cholesterol and Lipoproteins
There is abundant evidence linking lipids, cholesterol in particular, with atherosclerosis (2).
In 1913, Nikolai N. Anitschkow, a Russian pathologist in Saint Petersburg, demonstrated that when given to rabbits, cholesterol, extracted from the egg yolks, (purified, and dissolved in vegetable oil) produced arterial lesions that closely resembled those of human atherosclerosis (3).
Many autopsy studies have shown a relationship between the amount of blood cholesterol and the extent of atherosclerosis (4). Furthermore, accumulation of cholesterol is found in human atherosclerotic plaques (5).
Because fats are insoluble in water, cholesterol cannot be transported in blood on its own. Instead, cholesterol is attached to hydrophilic proteins that function as transport vehicles carrying different types of fats such as cholesterol, triglycerides, and phospholipids.
These combinations of fats and protein are termed lipoproteins. Lipoprotein particles vary in the primary lipoprotein present and the relative contents of the different lipid components.
There is strong evidence that lipoproteins play a fundamental role in atherosclerosis and their interaction with the arterial wall appears to initiate the cascade of events that leads to atherosclerosis.
There are five major types of lipoproteins; chylomicrons, very-low-density lipoprotein (VLDL), intermediate-density lipoprotein (IDL), low-density lipoprotein (LDL), and high-density lipoprotein (HDL).
Lately, the role of another lipoprotein, called lipoprotein(a) or Lp(a) has been highlighted (6).
Lipoproteins that promote atherosclerosis are termed atherogenic.
A specific protein, called Apolipoprotein B100 (ApoB), is an important component of all atherogenic lipoproteins (7).
Atherogenic lipoproteins such as LDL, VLDL, and Lp(a), all contain one ApoB molecule per particle. Hence, measurements of ApoB reflect the number of atherogenic particles.
On the other hand, HDL does not contain ApoB, and is not atherogenic. In fact, HDL appears to play a protective role and high levels of HDL particles are associated with less risk of coronary artery disease (9).
The LDL particle has a core that is mostly composed of cholesterol esters and a coat containing phospholipids and unesterified cholesterol. ApoB, the major protein moiety encircles the equator of the particle.
So, the atherogenicity of different lipoproteins is not determined by their cholesterol content. Instead, the lipoproteins’ molecular composition and the presence er absence of the ApoB molecule seem to be most important.
Lipoproteins are produced by the liver and their removal from the circulation is dependent on receptors found on the surface of cells, primarily in the liver. The LDL receptor plays a crucial role in the removal of LDL from the circulation.
Despite the proposed strengths of the associations between cholesterol, lipoproteins, and atherosclerosis, the underlying mechanisms have not been completely clarified.
Many people have high blood cholesterol throughout their lifetime without ever developing heart disease. Furthermore, a significant proportion of patients with coronary artery disease doesn’t have high blood cholesterol (10).
Retention of LDL in the Arterial Wall
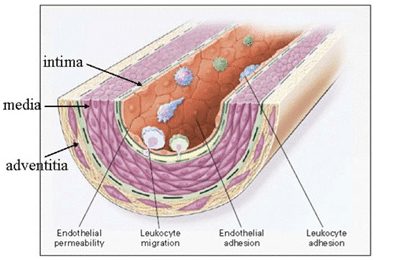
The wall of an artery consists of three layers, the tunica intima, the tunica media, and the adventitia. Also, there is the endothelium, a thin cellular layer that lines the interior surface of the artery.
The intima and media consist of smooth muscle cells and extracellular matrix. The outermost layer, the adventitia, consists of looser connective tissue, nerve endings, mast cells, and vasa vasorum (a network of small blood vessels that supply the walls of larger arteries).
An accumulation of LDL in the arterial intima is an early step in atherosclerosis. Increased permeability of the endothelium and increased intimal retention of LDL are critical elements in the process.
LDL particles interact with particular constituents of the intima, notably the extracellular matrix. Here, the presence of ApoB may be a key factor.
Chondroitin sulphate proteoglycans (11) produced by smooth muscle cells in the arterial wall interact with ApoB on the surface of lipoprotein particles, thereby increasing the retention of LDL.
Endothelial dysfunction may also be a key factor. It may cause increased permeability of the endothelium allowing atherogenic lipoproteins to enter the vessel wall.
However, if lipoproteins are not retained in the intima, atherosclerosis is less likely to occur. Therefore, factors that promote lipoprotein retention are likely to induce atherosclerosis.
LDL Particle Size and Atherosclerosis
The size of the LDL particles may influence how readily LDL penetrates the endothelial barrier. Small LDL particles appear to penetrate the the endothelium and reach the intima 1.7-fold more than large LDL particles (12).
Also, small, dense LDL particles are more likely to bind to proteoglycans than large fluffy LDL particles (13).
High numbers of small, dense LDL particles are associated with increased risk for CAD in prospective epidemiologic studies. (14).
Small LDL particles are associated with high triglycerides (15), low HDL cholesterol (9), insulin resistance, metabolic syndrome (16), and type 2 diabetes.
The propensity of small LDL particles to be retained within the intima may explain why patients with metabolic syndrome and type 2 diabetes are at heightened risk of coronary artery disease in the face of normal or average blood levels of LDL cholesterol.
Modified LDL (Glycated LDL and OxLDL) and Atherosclerosis
Evidence suggests that to initiate atherosclerosis, LDL has to undergo chemical modification. Otherwise, it can not unlatch the typical cellular and inflammatory reactions typical of the disorder.
The oxidation hypothesis of atherosclerosis, summarized in 1989 by Steinberg, Whitman, and colleagues, suggests that oxidative modification of LDL plays a crucial role (17).
At the most basic level, oxidation is the loss of electrons. When a compound is oxidized, its properties change.
Because of its complex composition, the LDL particle is very sensitive to oxidized damage.
Each LDL particle contains approximately 700 molecules of phospholipids, 600 molecules of free cholesterol, 1600 molecules of cholesterol esters, 185 molecules of triglycerides, and one molecule of apoB. Both the protein and lipid moieties can undergo oxidative modification.
Whereas circulating LDL is reasonably stable, the long dwelling time of LDL within the intima provides a greater opportunity for oxidative modification.
Recent findings suggest that oxLDL begins to deposit in human coronary arteries before plaque formation and increasingly deposits with plaque growth (18).
Plasma concentration of oxLDL is associated with the risk of acute coronary heart disease events (19). One study found that plasma oxLDL was the strongest predictor of such events compared with a conventional lipoprotein profile and other traditional risk factors (20).
Oxidized LDL (OxLDL) promotes the immune and inflammatory reactions that characterize atherosclerosis. Evidence suggests that these reactions may be genetically determined (21).
Glycation is another type of atherogenic modification of LDL that may contribute to atherosclerosis (22).
Glycation is the result of bonding of a protein or lipid molecule with a sugar molecule, such as fructose or glucose, without an enzyme’s controlling action.
Small, dense LDL is more susceptible to glycation than more buoyant LDL (23).
Glycation and oxidation of LDL appear to be intimately linked and glycated LDL is more likely to be oxidized than non-glycated LDL (24).
Inflammation and Atherosclerosis
Inflammation plays a vital role in the formation of atherosclerotic lesions and the subsequent clinical complications (25).
Popular theories on the initiation of atherosclerosis suggest that modified lipoproteins, such as oxLDL, may play a central role in promoting the inflammatory reactions that characterize and drive atherosclerosis.
Cytokines are small proteins that are important in cell signaling (26).
Common cytokines include interferons, adipokines, interleukins, and tumor necrosis factor.
The discovery that vascular wall cells themselves can produce cytokines provided an important insight into the initiation of atherosclerosis.
According to the original concept, cytokines function to signal between leukocytes (white blood cells), hence the name “interleukin” (27).
Products of oxLDL may stimulate vascular wall cells to produce cytokines (28). These cytokines are believed to be mediators of inflammation and immune reactions in the atherosclerotic process.
Leukocytes, the type of white blood cells which is typically involved in most inflammatory reactions in the body, appear to play a significant role in atherosclerosis.
Leukocyte recruitment to the arterial wall is an important initial step in the formation of atherosclerotic lesions. The circulating leukocytes that enter the vessel wall are called monocytes, but within tissues, they are termed macrophages.
Typically, the endothelium resists the adhesion of leukocytes derived from blood. However, when stimulated by pro-inflammatory cytokines, adhesion molecules on the surface of endothelial cells may capture leukocytes (29). Hence, cytokines may play a key role in recruiting inflammatory cells in the vascular wall.
Failure of counter-regulatory mechanisms may also promote inflammation and oxidation in atherosclerosis. For example, HDL particles may function as carriers for anti-inflammatory and antioxidant mediators (30). In fact, HDL is an effective antioxidant.
HDL may also inhibit the expression of adhesion molecules in endothelial cells, thus reducing the recruitment of leucocytes into the artery wall.
Furthermore, HDL can inhibit the oxidative modification of LDL and thereby reduce the atherogenic potential of LDL.
Hence, low HDL levels may aggravate atherosclerosis because of blunted anti-inflammatory and antioxidant actions.
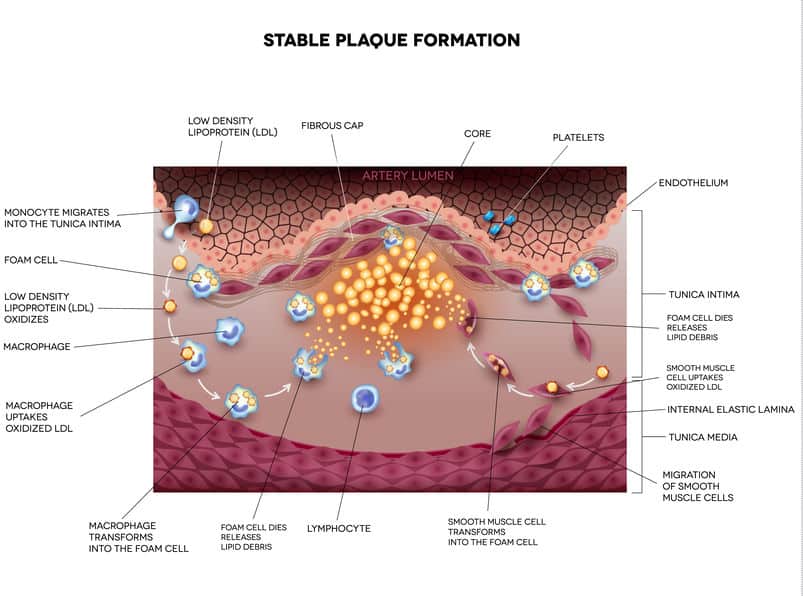
After reaching the intima, leukocytes (macrophages) take up modified lipoproteins. These-lipid laden white blood cells are called foam cells. Foam cells comprise the bulk of early atherosclerotic lesions, often termed fatty streaks (31).
Foam cells play a critical role in the occurrence and development of atherosclerosis.
The Stable Plaque and the Vulnerable Plaque
Rupture of the plaque surface, often with superimposed blood clotting (thrombosis), frequently occurs during the evolution of coronary atherosclerotic lesions.
Actually, plaque rupture is an important mechanism underlying most cases of acute heart attack and sudden cardiac death (32).
The concept of plaque rupture was first reported at the autopsy of the celebrated neoclassical Danish artist Bertel Thorvaldsen, who died of sudden cardiac death in the Royal Theater in Copenhagen in 1844 (33).
However, it was not until the next century that researchers described the features of plaques responsible for acute coronary syndrome and sudden cardiac death.
Atherosclerotic plaques may become large over time and bulge into the lumen of the artery, limiting blood flow to tissues and organs. However, these plaques are not necessarily prone to rupture because the risk of plaque rupture depends on plaque type (composition) rather than plaque size (volume).
An atherosclerotic plaque that is prone to rupture is defined as a vulnerable plaque, whereas a plaque that is not prone to rupture is considered a stable plaque.
A vulnerable plaque is characterized by a thin fibrous cap, large lipid-rich necrotic core, plaque inflammation, increased vasa-vasorum vascularization, and intra-plaque bleeding (34).
One of the most significant challenges facing atherosclerotic research is identifying how and why plaques become vulnerable and how this may be translated into clinical practice.
The Role of Metabolic Syndrome and Insulin Resistance
Lately, metabolic syndrome, obesity, and type 2 diabetes have become increasingly common. These disorders are characterized by insulin resistance and an increased risk of CAD (16).
Insulin resistance is associated with low blood levels of HDL-cholesterol and high levels of atherogenic triglyceride-rich lipoproteins such as VLDL (35).
Increased availability of small LDL particles is common in people with insulin resistance (36).
Furthermore, insulin resistance is associated with higher levels of circulating oxLDL, which may contribute to atherosclerosis and acute coronary events (39).
The Limitations of Using LDL-Cholesterol to Assess Risk
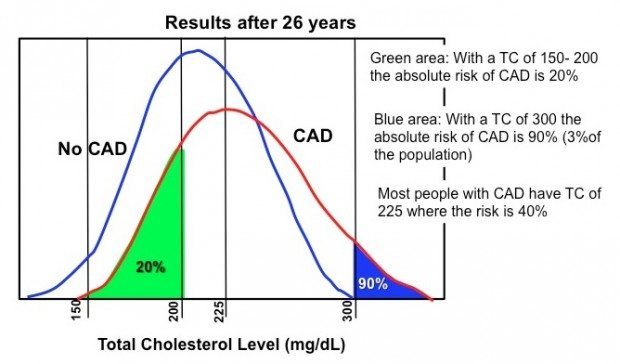
The figure below is based on data from the Framingham Study showing the distribution of blood cholesterol in people with and without CAD (37). Both curves are bell-shaped with the top of the bell corresponding to the medium cholesterol level in each group.
Castelli, William. The American Journal of Cardiology, 1998: 82:60T-65T
Notice that those who have coronary artery disease have slightly higher medium levels of blood cholesterol, but the difference is small.
Interestingly, a substantial number of people with normal cholesterol levels (<200 mg/dL) develop coronary artery disease. Furthermore, a significant number of individuals with elevated cholesterol (225-300 mg/dL) don’t have coronary artery disease.
Blood levels of LDL-cholesterol are commonly used to assess the risk of heart disease. However, using LDL-cholesterol to assess risk has several limitations (38).
The LDL-cholesterol value accounts for the total amount of cholesterol carried by LDL particles. Importantly, it doesn’t account for the number of LDL particles present in the circulation, which is more important when it comes to risk assessment (39).
Furthermore, LDL-cholesterol does not provide information about the size of LDL particles, which is important because small particles are more strongly associated with atherosclerosis than large particles.
So, of course, high blood cholesterol is not enough to cause atherosclerosis. But, if the availability of atherogenic lipoproteins such as LDL and VLDL is high, atherosclerosis is more likely to occur. However, for that to happen, other factors have to be present as well.
Lately, metabolic syndrome, obesity, and type 2 diabetes have become increasingly common. These disorders are characterized by insulin resistance and an increased risk of CAD.
A Few Practical Considerations
During the last 75 years, a simplified model of atherosclerosis and heart disease has been presented to health professionals and the lay public.
The model higlights cholesterol accumulation in the vessel wall as the main culprit. Consequently, lifestyle measures that lower cholesterol are emphasized.
Clinical and dietary guidelines have pinnacled LDL-cholesterol as an important target to prevent the occurrence of CAD.
Recommendations to limit the intake of saturated fats and cholesterol are based on the assumption that these types of fats will raise LDL-cholesterol and thereby increase risk. Hence, low-fat food products have been marketed with the aim of reducing the burden of cardiovascular disease.
Nonetheless, compared with low-fat diets, low-carbohydrate diets provide greater improvements in parameters associated with insulin resistance, such as HDL cholesterol, VLDL, LDL particle size, and particle number (40).
Moreover, low-carbohydrate diets provide greater reductions in inflammatory markers than low-fat diets (41).
There is no reason to believe that food products that elevate HDL cholesterol, lower triglycerides, reduce the availability of atherogenic LDL particles, and reduce insulin resistance and inflammatory markers, would be less effective in fighting heart disease than food that lowers LDL cholesterol.
That’s not to say that cholesterol doesn’t matter.
Lowering the availability of cholesterol-rich lipoproteins such as LDL and VLDL may be crucial in patients with coronary artery disease and individuals prone to atherosclerosis, such as those with familial hypercholesterolemia.
Denying the role of cholesterol in atherosclerosis is as naive as believing it explains everything.
Summary
An accumulation of LDL in the arterial wall is an essential step in the initiation of atherosclerosis.
Increased permeability of the endothelium and increased retention of LDL particles within the intima are important underlying mechanisms.
Small LDL particles are more likely to be retained in the intima than large buoyant LDL particles.
LDL particles may undergo chemical modification within the intima and become oxidized. OxLDL may enter white blood cells (leukocytes) called macrophages, which subsequently transform into foam cells. Foam cells are commonly found in atherosclerotic plaques.
Products of oxLDL may provoke vascular wall cells to produce cytokines, which promote recruitment of inflammatory cells into the vascular wall. Immune reactions and low-grade inflammation play a crucial role in the formation and progression of atherosclerotic plaques.
Rupture of the plaque surface, often with superimposed blood clotting (thrombosis), frequently occurs during the evolution of coronary atherosclerotic lesions. Plaque rupture is an important mechanism underlying most cases of acute heart attack and sudden cardiac death. Plaques that are prone to rupture are termed vulnerable plaques.
Currently, atherosclerosis is viewed as a complex multifactorial disorder involving the vessel wall, endothelial function, lipoproteins, lipoprotein modification such as glycation and oxidation, immune reactions, inflammation, and blood clotting (thrombosis).
It is the responsibility of experts in the field to educate health professionals and the general public about the complexity of atherosclerosis.
Unfortunately, the deep-rooted and oversimplified cholesterol-model of atherosclerosis has skewed recommendations on dietary interventions and other lifestyle measures to prevent coronary artery disease.
The article was initially published in 2016.
It was revised, updated and republished on February 13th, 2021.
Have you ever experienced or sensed your heartbeat?
Although such a sensation is usually completely normal, it may be unpleasant. For instance, people often describe hard beats, fast beats, irregular beats, skipped beats, fluttering, “flip-flopping” or a pounding sensation in the chest or neck.
The term palpitations is used to describe an unpleasant awareness of the forceful, rapid, or irregular beating of the heart (1).
Although palpitations are very common and most often completely harmless, they may occasionally be a manifestation of underlying heart disease.
People often seek medical advice because of palpitations. This is not surprising as symptoms associated with the beating of the heart are likely to get our attention and they often make us anxious.
However, keep in mind that palpitations are more often caused by anxiety itself than underlying heart disease.
The key thing is to understand that palpitations are a subjective symptom, an experience, or a sensation. As such they may be difficult to grade or measure. Furthermore, the description often varies a lot between individuals.
While some people seem to be aware of their heartbeat at all times, others rarely feel their heart beating. Obviously, the latter group is less likely to complain of palpitations.
What Causes Palpitations?
The term arrhythmia describes disorders of heart rhythm. All types of irregular or abnormal heart rhythms fall under this term. It may be an irregular rhythm or a rapid or slow beating of the heart.
The term tachycardia describes rapid beating of the heart whereas the term bradycardia describes slow heart rate.
Although palpitations are often caused by arrhythmia, they are frequently associated with psychiatric causes such as anxiety and panic disorders (2).
Other underlying disorders such as thyroid disease or anemia (low blood count) may also cause palpitations.
Emotional stress and lack of sleep may also play a role. Sometimes substances like caffeine, nicotine, cocaine, or amphetamine are identified as the main cause.
Interestingly, palpitations can occur in the absence of arrhythmia. Furthermore, many patients with arrhythmia don’t have palpitations (3).
Palpitations are sometimes caused by underlying heart disease. Examples are valvular heart disease, coronary heart disease, or disease of the heart muscle (cardiomyopathy).
The Conduction System of the Heart
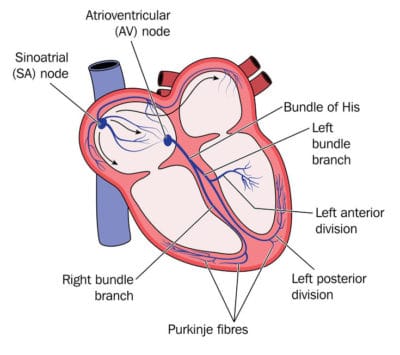
To understand the underlying mechanisms causing arrhythmias, it is helpful to understand the basics of the electrical conduction system of the heart.
The heart’s physiological pacemaker also called the sinus node (SA node), is located in the right upper chamber of the heart, the right atrium.
The conduction system of the heart.
Normal heart rhythm originating from the sinus node is termed sinus rhythm.
The sinus node emits more than 2.5 billion electric pulses during a lifetime.
Each time the sinus node generates a new electrical impulse; that impulse spreads out through the conduction system of the heart.
First, the electrical signal travels through the two upper chambers of the heart, the atria, causing them to contract and eject blood into the left and right ventricles.
Next, the signals travel to the area that connects the atria with the lower chambers of the heart (the ventricles), the atrioventricular node (AV node), and from there through an area called the AV bundle or the bundle of His.
The bundle of His splits into thinner branches (right and left bundle branches) that extend to the right and left ventricles. Finally, the signals reach the muscle cells of the ventricles, causing them to contract.
A normal resting pulse usually varies between 40 to 100 per minute. The sinus node, influenced by signals from the nervous system and endocrine organs, constantly adjusts the heart rate to meet demands such as during physical exercise
Palpitations and Arrhythmia
Sometimes a completely normal sinus rhythm is associated with palpitations, underscoring the fact that palpitations are not always caused by arrhythmia.
However, electrical impulses not originating from the sinus node frequently cause palpitations. This may lead to so-called ectopic or premature beats.
Atrial and so-called supraventricular premature beats originate from the atria or the atrioventricular node.
The term ‘supraventricular’ means ‘above the ventricles’.
Ventricular premature beats are due to ectopic electric activity originating from the ventricles.
Ventricular premature beats are easily detected on an ECG
Ventricular and supraventricular premature beats are the most common underlying arrhythmias causing palpitations (3).
Such premature beats are usually not caused by underlying heart disease. Hence, patients suffering from such arrhythmias usually have an excellent prognosis.
Sometimes bouts of rapid, repeated ventricular or supraventricular beats may cause palpitations. These are termed ventricular tachycardia and atrial or supraventricular tachycardia respectively.
Ventricular tachycardia may cause dizziness and fainting. The prognosis is usually good if it lasts less than 30 seconds (non-sustained) and is not associated with underlying heart disease.
However, ventricular tachycardia may sometimes be associated with adverse prognosis and risk of sudden death.
Supraventricular tachycardia is relatively common. Although the prognosis is usually good, this arrhythmia commonly causes palpitations, and specific treatment may be needed to relieve symptoms.
Atrial fibrillation is a common underlying cause of palpitations (5). It is characterized by a chaotic electrical activity of the atria leading to rapid, irregular heart rhythm. Atrial fibrillation is sometimes associated with an increased risk of stroke.
Evaluation of Patients With Palpitations
Because palpitations may occasionally reflect severe underlying heart disease, an evaluation by a doctor is usually recommended.
However, because most people with palpitations have a good prognosis, intensive, expensive testing is usually not necessary.
In one study of people with palpitations, the 1-year mortality rate was 1.6%, and those who died were all over age 70 and none of the deaths was believed to be related to the origin of the palpitations (6)
The most important thing when addressing patients with palpitations is to exclude underlying heart disease.
All patients should be evaluated by detailed history, physical examination,and an electrocardiogram (ECG).
History and Physical Examination
The characteristics of the palpitations are essential.
Does the patient describe fast beats, skipped beats, or flip-flopping? Is the rhythm regular or irregular? Are there any associated symptoms such as dizziness, fainting or shortness of breath, or chest pain? Are palpitations present at rest, during exercise, or both? Are palpitations present when the patient lies on his left side?
The flip-flopping sensation is usually caused by atrial or ventricular premature beats and is therefore usually benign. This type of palpitations is often experienced while the patient is lying in bed.
Palpitations are often more easily felt when lying on the left side.
When lying on the left side, the apex of the heart is closer to the chest wall which may lead to more awareness of the heart. Hence, palpitations while lying on the left side is usually a completely innocent phenomenon. The simplest measure to get rid of it is to change position.
Rapid fluttering in the chest is likely to be caused by tachycardia. If it is regular, it may indicate supraventricular or ventricular tachycardia but if it is irregular, it may suggest atrial fibrillation.
The age of the patient is important. For example, rapid heart rate at a young age is likely to be caused by a supraventricular tachycardia, while, as the subject ages, such symptoms are more likely to be caused by atrial fibrillation.
Although serious ventricular arrhythmias typically occur in older patients with underlying heart disease, they may occasionally occur in adolescence, sometimes due to congenital long QT syndrome (7).
Sometimes patients become adept at terminating their palpitations by specific maneuvers, such as the so-called Valsalva maneuver. This mode of termination may suggest supraventricular tachycardia as the underlying disorder (1).
Palpitations associated with fainting may suggest more serious arrhythmias such as ventricular tachycardia.
It is important to know about all medication taken by the patient. For example, palpitations may occur with some drugs taken for relieving asthma and cold and cough medications that contain pseudoephedrine. Furthermore, nicotine and illicit drugs such as cocaine or amphetamine may cause palpitations.
The patient should also be evaluated for other possible medical conditions. Laboratory testing for anemia (low blood count) and possible thyroid disease may be indicated.
Physical examination is useful for identifying abnormalities that may be associated with palpitations. For example, it may help detect congenital and valvular heart disease, chronic atrial fibrillation, and thyroid disease.
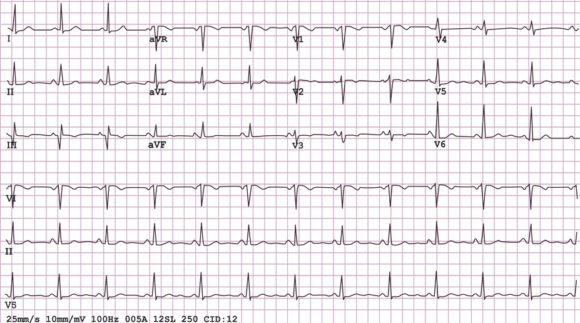
Electrocardiogram (ECG)
An ECG is a noninvasive test where electrodes are placed on the chest and extremities for registration of the electric activity of the heart.
The ECG may directly detect the underlying arrhythmia causing the palpitations. However, because palpitations are usually intermittent, the ECG is most often completely normal.
In some cases, the ECG may suggest underlying heart diseases such as coronary heart disease or a thickened and strained heart muscle (left ventricular hypertrophy).
Sometimes isolated premature ventricular or supraventricular beats may be seen on the ECG, thus suggesting the underlying cause of the palpitations. Prolongation of the QT-interval on the ECG may suggest congenital long-QT syndrome (7).
A 12-lead electrocardiogram (ECG) is an important diagnostic tool when evaluating patients with palpitatins.
Further Diagnostic Testing
When history, physical examination, and ECG do not provide a definitive diagnosis, further diagnostic testing may be warranted.
Sometimes further testing is needed to exclude underlying heart disease. It may also be performed to identify a treatable condition, thus improving the patient’s quality of life or simply to reassure the patient.
Echocardiography
Echocardiography is a non-invasive examination of the heart. It provides images of the heart’s structure and function and can help identify underlying heart disease.
Ambulatory ECG monitoring
Ambulatory ECG monitoring devices are important tools for the diagnosis of palpitations (8).
The Holter monitor is a portable device that records and saves data. It is usually worn for one to three days and sometimes up to a week. At the same time, the patient keeps a diary of his/her symptoms. This may help to detect or exclude arrhythmia associated with the palpitations.
Smartphones are becoming frequently used for ECG monitoring
Special loop event recorders can save data for longer periods of time and direct transmission of signals may be possible through telephone (9).
The implantable loop recorder (ILR) is implanted under the skin and can be used for much longer time periods. It is most often used in patients with unexplained fainting but also on rare occasions for unexplained palpitations (10).
Today, different types of smartphone apps are becoming frequently used to detect arrhythmia in patients with palpitations (11).
Management of Palpitations
As most patients with palpitations have an excellent prognosis, reassurance is often the most important and the only therapeutic measure needed.
If there are no signs of underlying heart disease or other associated conditions, specific treatment is usually not warranted.
However, due to the frequent association between anxiety disorders and palpitations, a psychiatric or psychological evaluation may sometimes be warranted.
If arrhythmia or another underlying disorder is detected, treatment will depend on the nature of that particular disorder.
The Take-Home Message
Palpitations are an unpleasant awareness of heart muscle contractions in the chest.
Although palpitations are very common and usually completely harmless, they may occasionally be a manifestation of underlying heart disease.
Although palpitations are sometimes caused by irregularities of heart rhythm (arrhythmia), they are often associated with anxiety and panic disorders.
Ventricular and atrial or supraventricular premature beats are the most common arrhythmia causing palpitations. Although they may cause unpleasant symptoms, they are usually harmless.
The key issue when addressing patients with palpitations is to exclude serious arrhythmias or underlying heart disease. This may usually be done by a careful history, physical examination, and ECG.
Ambulatory ECG monitoring is a useful tool to detect disorders of heart rhythm.
As most patients with palpitations have an excellent prognosis, reassurance is often the most important and the only therapeutic measure needed.
If arrhythmia or another underlying disorder is detected, treatment will depend on the nature of that particular disorder.
The article was initially published in 2015.
It was revised, updated and republished on January 24th, 2021.