
Most experts agree that diet is an important modifiable risk factor for cardiovascular disease and many other chronic noncommunicable disorders. Hence, defining and implementing a healthy diet is a matter of great public health interest. However, although there is substantial agreement on many issues, such as the importance of fruits and vegetables, several matters are still subjects of considerable controversy.
The World Health Organization (WHO) recommends that total fat should not exceed 30% of total energy intake to avoid unhealthy weight gain with a shift in fat consumption away from saturated fats to unsaturated fats and towards the elimination of industrial trans fats (1).

The importance of lowering the intake of saturated fat and replacing it with unsaturated fat, especially polyunsaturated fats was recently highlighted by a Presidential Advisory from the American Heart Association (AHA) (2). The main argument was that such a measure would “lower low-density lipoprotein cholesterol, a cause of atherosclerosis, linking biological evidence with the incidence of cardiovascular disease in populations and clinical trials”.
However, a growing number of scientists claim that the advice to restrict saturated fatty acids “is largely based on a selective emphasis on some observational and clinical data, despite the existence of several randomized trials and observational studies that do not support these conclusions” (3).
All these issues were recently highlighted by the publication of the PURE study on fat and carbohydrate intake (4,5).
The authors of the paper, lead by Mahshid Dehghan, concluded that high carbohydrate intake (more than about 60% of energy) was associated with an adverse impact on total mortality and non-cardiovascular disease mortality.
By contrast, higher fat intake was associated with lower risk of total mortality, non-cardiovascular disease mortality, and stroke. Furthermore, higher intakes of individual types of fat were associated with lower total mortality, non-cardiovascular disease mortality, and stroke risk and were not associated with risk of major cardiovascular disease events, myocardial infarction, or cardiovascular disease mortality.
Our findings do not support the current recommendation to limit total fat intake to less than 30% of energy and saturated fat intake to less than 10% of energy. Individuals with high carbohydrate intake might benefit from a reduction in carbohydrate intake and increase in the consumption of fats.
These conclusions initially appeared to shake up the world of nutrition and cardiovascular science. But, now, when the dust has settled, things seem calm as a millpond. It’s almost as if Dehghan and coworkers have had a firm slap on the wrist.
It has even been suggested by leading public health authorities that a closer look at the PURE results will reveal they do indeed not support the conclusion that nutritional advice should change (6).
Interestingly, The European Heart Network, which plays a leading role in the prevention and reduction of cardiovascular diseases in Europe, concluded that it would not be prudent to draw conclusions on what sort of level of intakes of fat, including saturated fat, and carbohydrates should be recommended for Europeans on the basis of the PURE study (7).
However, some experts see things differently. Dr. Dariush Mozaffarian, the dean of the Tufts Friedman School of Nutrition Science and Policy, said: “The PURE results provide strong support for evidence accumulating over the past decade on what makes a healthy diet. Cutting back on starch and sugar and adding more fat and more foods from plants, especially bioactive fruits and seeds, is where we should be headed (8).”
Personally, I tend to agree with Dr. Mozaffarian and I think it is imperative that the PURE data won’t be swept under the rug. However, it is important to listen to opposing arguments and those who claim that nutritional advice should remain unchanged despite PURE (or even because of PURE for that matter).
The PURE Study – A Few Opposing Arguments
The PURE study addressed the dietary intake of 135.535 individuals in 18 countries who were followed for a median of 7.4 years. The aim was to include populations that varied by socioeconomic factors. There were three high income (Canada, Sweden, and the United Arab Emirates), 11 middle income (Argentina, Brazil, Chile, China, Colombia, Iran, Malaysia, occupied Palestinian territory, Poland, South Africa, and Turkey), and four low-income countries (Bangladesh, India, Pakistan, and Zimbabwe).
The authors analyze their data by dividing macronutrient consumption into quintiles. Hence, the quintile 1 category includes the 20% with the lowest consumption and the quintile 5 category includes the 20% with the highest consumption.
Interestingly, the lowest quintile category was used as a reference group for the statistical analyses. Some experts believe this may have led to wrong conclusions. In fact, the relationship between the consumption of saturated fats and cardiovascular risk may be U-shaped and not linear. In quintile 1, which had the highest mortality, the mean consumption of saturated fat was only 2.8% of energy intake. It is argued that so little saturated fat is rarely consumed in high-income countries like the USA for example.
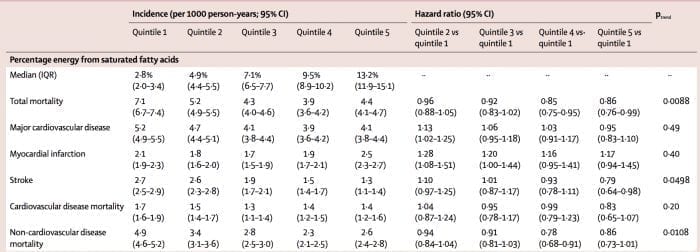
If we look at total mortality and myocardial infarction we can see that the relationship between saturated fat consumption and clinical outcome may indeed be U-shaped. The risk is highest in quintile 1, then goes down, and starts to increase again in quintile 5 where saturated fat consumption was highest.
Using quintile 1 as a reference for the statistical comparison might be similar to using the group with the lowest BMI (body mass index) when addressing the relationship between BMI and clinical outcome. It is well known that low BMI is associated with increased risk.
So, what happens if we skip quintiles 1 and 2 because these are not applicable to western countries, and only look at total mortality, major cardiovascular disease, and myocardial infarction? In fact, we will see that quintile 3 and 4, where mean saturated fat consumption was 7.1% and 9.5% respectively, did best in terms of the clinical outcome.
However, apparently, this approach cannot explain the inverse relationship between saturated fat consumption and the risk of stroke. The more saturated fat consumed, the less the risk of stroke. I have a hard time understanding how these results may be disregarded.
It has been pointed out that total fat consumption in the lowest quintile was only about 11% of energy intake. Numbers that low are probably very uncommon in high-income countries.
In the highest quintile, which seems to do best in terms of risk, mean fat consumption was 35% of total energy intake which is above the WHO recommendation but in line with guidelines in many countries, including the Nordic countries, where the recommended fat consumption is 25-40% of energy intake. So, here it may be argued that the PURE results are concordant with current dietary advice.
Health authorities usually recommend that carbohydrate consumption should be between 45-60% of energy intake. In the lowest quintile in PURE which fared best in terms of risk, mean carbohydrate consumption was 46% of energy intake. However, mean carbohydrate consumption in quintiles 4 and 5 was, 68% and 77% respectively. While such a high carbohydrate consumption was associated with worse clinical outcome, it has been argued that it is probably uncommon in high-income countries.
The Takeaway
Many experts believe the PURE study is fraught with methodological problems, not least because of different degrees of socio-economic development in different countries.
According to the European Heart Network: “There are significant differences between diets in high-income countries and low and middle-income countries. There are also significant socio-economic differences, e.g., general health status and access to health care. Additionally, we take note that the study does not distinguish between different types of carbohydrates, i.e., complex carbohydrates rich in fiber are not distinguished from simple carbohydrates, e.g., sugars”.
Obviously, the inability to differentiate between the types of carbohydrate is a significant issue when interpreting the PURE data.
Another thing that has to be acknowledged in PURE is possible social desirability bias. In other words, individuals who are health conscious are more likely than others to adopt a healthy lifestyle. However, as the authors point out, if this were the case, there would not be different associations for different outcomes.
Furthermore, residual confounding may affect the results. Hence, the ability to afford certain foods may change the dietary pattern. For example, high-carbohydrate and low-fat diets may be associated with poverty.
However, the authors of the PURE paper point out that additional analyses adjusting for other measures of socioeconomic status (household, wealth or income) did not alter the results. Of course, the possibility of residual confounding can never be completely ruled out by such measures.
In another recently published study by the PURE investigators, it was concluded that reducing saturated fatty acid intake and replacing it with carbohydrate has an adverse effect on blood lipids. Substituting saturated fatty acids with unsaturated fats might improve some risk markers, but might worsen others. Simulations suggest that ApoB-to-ApoA1 ratio probably provides the best overall indication of the effect of saturated fatty acids on cardiovascular disease risk among the markers tested. Focusing on a single lipid marker such as LDL cholesterol alone does not capture the net clinical effects of nutrients on cardiovascular risk (9).
The PURE study leaders believe that global dietary guidelines should be reconsidered in light of the consistency of their findings together with meta-analyses of other observational studies and the results of recent randomized trials (10). However, it is quite obvious that these conclusions have not been embraced by leading public health experts in western countries.
Let me finish by Ramsden’s and Domenichiello’s final conclusion from their recent editorial published in The Lancet (3):
“The PURE study is an impressive undertaking that will contribute to public health for years to come. Initial PURE findings challenge conventional diet-disease tenets that are largely based on observational associations in European and North American populations, adding to the uncertainty about what constitutes a healthy diet. This uncertainty is likely to prevail until well designed randomized controlled trials are done. Until then, the best medicine for the nutrition field is a healthy dose of humility.”
I’ve read sat fat increases the good apo A1. hDL. Loses lpa and raises ldl particle size size with ldl overall numbers. With what looks to be optimal levels of 7-9 percent of overall fat intake ( is that ideally 30%) of overall calories in a day in addition which types sat fat are best. I’ve been hooked on chocolate from all the supposed health benefits of it but have recently discovered the stearic acid component of cocoa butters’ saturated fat profile tstcwasakeays deemed to healthy and cholesterol neutral apparently is a problem after all. It’s one of only fats that raises lpa and it seems the highest intake of stearic acid around 9 grams a day ( with average intake is 3 grams a day ) cvd risk increases.
Can you elaborate of this. Stearic acid was always said to be cholesterol neutral or even lowering. What’s even more odd is that stearic acid converts to oleic acid quickly so does that mean olive oil isn’t really cholestrol beneficial abd could also raise lpa?