
Obstructive sleep apnea (OSA) is a relatively common sleep disorder with several potentially serious consequences. It causes breathing to stop and then start again intermittently during sleep.
The word apnea describes suspension of breathing.
OSA may seriously affect quality of life and is strongly associated with the risk of diabetes, high blood pressure, liver disorders, and cardiovascular disease.
Treatment of OSA usually improves well-being and reduces the risk of associated disorders.
However, many people with OSA don’t receive treatment because they are not properly diagnosed.
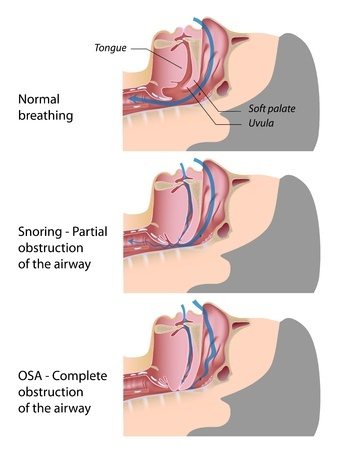
There are several types of sleep apnea, but OSA is the most common. OSA occurs when the throat muscles intermittently relax and block the airways during sleep causing a repetitive obstruction of the upper airway during sleep.
 The Pickwick Papers and the Pickwickian Syndrome
The Pickwick Papers and the Pickwickian Syndrome
In his novel, The Pickwick Papers published 1836, English writer Charles Dickens writes about Joe, a fat, red-faced boy who suffered from severe daytime sleepiness.
Dickens introduces Joe by these words: “And on the box sat a fat and red-faced boy in a state of somnolence.”
And, it is true that OSA is very often associated with obesity. Obesity is the biggest risk factor for the disorder. Obese individuals often have enlargement of soft tissue within and surrounding the airways. They may be able to compensate for the upper airway narrowing during wakefulness, but this protective effect is lost during sleep when relaxation of the muscle occurs.
Patients with OSA often suffer from daytime sleepiness and snoring. Dickens wrote: “Sleep!” said the old gentleman, ‘he (Joe) is always asleep. Goes on errands fast asleep, and snores as he waits at table.”
Later, the term Pickwickian syndrome was used to describe a condition in which severe obesity leads to a failure of the person to breathe efficiently, resulting in low levels of oxygen in the blood and high levels of carbon dioxide.
Everything suggests that Joe, the young lad, suffered from OSA.
How Common Is Obstructive Sleep Apnea?
Recent estimates suggest that the prevalence of OSA has increased substantially over the last two decades.
The estimated prevalence among US adults is approximately 20 to 30 percent in males and 10 to 15 percent in females when OSA is defined broadly. If more stringent criteria are used, roughly 13 percent of men and 6 percent of women have moderate or severe OSA (1).
The increased prevalence of obesity is believed to be responsible for the increasing number of people with OSA. It is estimated that 50 to 60 percent of people who are obese or have metabolic syndrome also have OSA (2).
OSA is approximately two to three times more common in males than females, although the gap narrows at the age of menopause in women (3).
Relatively few people with symptomatic OSA receive a diagnosis of OSA and even fewer receive treatment (4).
Symptoms of Obstructive Sleep Apnea
Persons with OSA commonly experience loud snoring, choking or gasping during sleep, low oxygen saturation in blood, and disruption of sleep.
Disrupted sleep can result in excessive daytime sleepiness, somnolence, and impaired concentration during the day.
Snoring
Snoring is a common feature of OSA. However, although 80 to 90 percent of people with OSA report snoring, many people who snore don’t have OSA.
It is often helpful to ask the patient’s bed partner about the magnitude of snoring because he/she may provide greater insight than the patient into the amount of the snoring, as well as events such as gasping or periods of silence followed by loud snoring.

Daytime Sleepiness
Daytime sleepiness is a key feature of OSA.
However, it is important to acknowledge the difference between daytime sleepiness and fatigue.
Sleepiness is the inability to remain fully awake or alert during the day while fatigue is a subjective lack of physical or mental energy interfering with daily activities.
Sometimes people with sleepiness use terms like fatigue, tiredness, and low energy to describe their symptoms.
However, careful questioning usually reveals a pattern of feeling sleepy or falling asleep in boring or passive situations. The patient may easily fall asleep while reading and watching television.
OSA is associated with an increased risk of falling asleep while driving. Therefore, the risk of traffic accidents is increased (5,6).
High Blood Pressure (hypertension)
There is a strong association between OSA and hypertension (7).
The relationship between high blood pressure and OSA is believed to be due to many factors. Sympathetic overactivity, oxidative stress, and endothelial dysfunction may all play a role.
Treatment of OSA by CPAP (continuous positive airway pressure) may lower blood pressure in people with OSA and hypertension (8,9).
Type 2 Diabetes
An association between OSA, insulin resistance, and type 2 diabetes has been consistently demonstrated (10,11).
Evidence suggests that the intermittent lowering of oxygen saturation (hypoxia) may harm the beta cells of the pancreas, thereby increasing the risk of diabetes (12,13).
Nonalcoholic Fatty Liver Disease (NAFLD)
Although nonalcoholic fatty liver disease (NAFLD) is associated with obesity, the underlying mechanisms are not entirely understood.
There is evidence suggesting that OSA may increase the risk of NAFLD in people with obesity (14). It has been suggested that intermittent fall in blood oxygen levels in OSA may damage liver cells and exacerbate NAFLD in individuals with obesity (15).
Atrial Fibrillation
Atrial fibrillation is the most commonly encountered arrhythmia in clinical practice and a major cause of morbidity and mortality. Over 2 million adults in the US have atrial fibrillation (16).
A strong association between OSA and atrial fibrillation has been consistently observed in both epidemiological and clinical cohorts (17).
Obesity and the severity of nighttime hypoxia, are independent risk factors for atrial fibrillation (18).
Treatment of OSA with CPAP appears to reduce the recurrence of atrial fibrillation (19).
Diagnosing Obstructive Sleep Apnea
The challenge is to select the patients who are most likely to have OSA for further testing since expensive and time-consuming testing has traditionally been required to identify OSA.
Questionnaires are often used to screen individuals for further diagnostic evaluation. The most commonly used is test the Epworth Sleepiness Scale (ESS) (20).
Polysomnography is considered the reference standard for diagnosing OSA. However, it requires specialized resources, is expensive and has to be performed in a sleep laboratory setting.
Out-of-center sleep testing (OCST) or portable monitoring is an unattended monitoring of cardiorespiratory parameters during sleep. There is a wide variety of devices available many of whom have been validated against standard polysomnography.
The diagnosis of OSA is based on the presence or absence of related symptoms, as well as the frequency of respiratory events during sleep as measured by polysomnography or OCST.
The Disease Spectrum
The apnea-hypopnea index (AHI) represents the number of apnea (complete cessation of breathing) and hypopnea (partial obstruction) events per hour of sleep. An AHI of less than five is considered normal.
Patients with OSA are traditionally classified as having mild, moderate or severe disease based on symptoms and the AHI.
Mild OSA: An AHI between 5 and 15 respiratory events per hour of sleep. This is usually associated with mild symptoms.
Moderate OSA: An AHI between 15 and 30 respiratory events per hour of sleep. Such patients typically experience daytime sleepiness, and they may have an increased incidence of motor vehicle violations or accidents.
Severe OSA: An AHI greater than 30 respiratory events per hour of sleep and/or an oxyhemoglobin saturation below 90 percent for more than 20 percent of the total sleep time. Such patients usually have daytime sleepiness that interferes with normal daily activities. They tend to fall asleep often during the day and are at risk for accidental injury. Patients with severe OSA are at increased risk for all-cause mortality, high blood pressure, coronary artery disease, and arrhythmias.
Treatment of Obstructive Sleep Apnea
Untreated OSA has many potential consequences and is associated with adverse clinical outcomes including excessive daytime sleepiness, cognitive impairment, increased risk of diabetes, high blood pressure, and atrial fibrillation.
General measures
OSA should be approached as a chronic disorder that requires long-term, multidisciplinary management. Therefore, apart from treating OSA itself, lifestyle modification and treatment of other risk factors is of crucial importance.
The goals of OSA therapy are to resolve signs and symptoms of OSA, improve sleep quality, normalize the AHI, and improve oxygen saturation of blood during sleep.
Sleep position may play a role. Some patients have OSA that develops or worsens during sleep in the supine position. Such patients usually have less severe OSA and sleeping in a non-supine position may improve their symptoms.
Weight loss and exercise should be recommended to all patients with OSA, who are overweight or obese. Weight loss has been shown to improve overall health and metabolic parameters, decrease the AHI, reduce blood pressure, improve the quality of life, and decrease daytime sleepiness (21,22,23).
It is reasonable to recommend all patients with untreated OSA to avoid alcohol as it can exacerbate OSA, worsen sleepiness, and promote weight gain. Acute alcohol consumption usually worsens the duration and frequency of sleep apnea (24).
Positive Airway Pressure Therapy
Positive airway pressure therapy is the mainstay of treatment for adults with OSA.
The method uses mild air pressure to keep the airways open. The patient uses a mask that fits over the nose or the nose and mouth. Straps keep the mask in place. A tube connects the mask to a machine that blows air into the tube.
The mechanism of involves maintenance of a positive pharyngeal transmural pressure so that the pressure within the airways exceeds the surrounding pressure. As a result, respiratory events due to a collapse of the upper airways are prevented.

There is very strong evidence from randomized trials that positive airway pressure therapy reduces the frequency of respiratory events during sleep, decreases daytime sleepiness, lowers blood pressure, and improves the quality of life (25,26,27, 28).
Oral Appliances
There are an increasing number of oral appliances that are designed to either protrude the chin bone (mandible) forward or hold the tongue in a more forward position. This may help maintain the potency of the upper airways.

Oral appliances may be offered to patients with mild to moderate OSA who decline or fail to adhere to positive airway pressure therapy and who have a preference for such treatment.
Upper Airway Surgery
There is no consensus regarding the role of surgery in patients with OSA, nor have optimal screening or imaging procedures been established that accurately predict which patients are most likely to benefit from surgery.
Surgical treatment appears to be most effective in patients who have OSA due to a severe, surgically correctable, obstructing lesion of the upper airway.
Surgical therapy is often considered when positive airway pressure or an oral appliance is declined or ineffective.
A variety of surgical procedures is available for the treatment of OSA in patients without a discrete anatomic lesion obstructing the upper airway. However, the efficacy of these procedures has not been extensively studied.
The Take Home Message
Due to the rapidly increasing prevalence of obesity, OSA is becoming more common.
Apart from adversely affecting the quality of life, OSA is strongly associated with the risk of diabetes, high blood pressure, liver disorders and cardiovascular disease.
Many people with OSA don’t receive treatment because they are not properly diagnosed.
A recent systematic review of available data suggests that positive airway pressure therapy (PAP), which is the most commonly used treatment modality, does not reduce the risk of cardiovascular outcomes or death in patients with OAS (29).
However, PAP is effective in reducing symptoms of sleepiness and improving quality of life measures in people with moderate and severe OAS.
OSA should be approached as a chronic disorder that requires long-term, multidisciplinary management. Therefore, apart from treating OSA itself, lifestyle modification and treatment of other risk factors are of crucial importance.
Unfortunately, your last sentence isn’t supported by the available data, according to this just published meta-analysis: https://jamanetwork.com/journals/jama/article-abstract/2643307
Thanks Jim for drawing my attention to this important paper. I do appreciate it. I’ve changed my conclusions accordingly.
Yourself and your followers have the open option to read into the Theory of Earthing and thence consider what it’s authors, proponents, and persons who have adopted the practice have to say on the matter of OSA (and other troublesome conditions).
Begin: https://www.earthinginstitute.net/
The benefits of earthing are something everybody enjoyed without taking any special steps or initiatives and without being aware right up until the time rubber and plastics arri9ved on the scene became the materials of choice for the manufacture of soles for our footwear. This innovative step made possible by perfecting polymer and vulcanisation technologies projected humans into a state of almost total isolation from ‘ground’ (‘isolation’ and ‘ground’ both terms used, quite intentionally, with their electrical connotations firmly attached).
One wouldn’t (or might not rush to) think this level of isolation matters. However it does go against natures precedents; the wearing of shoes is rare amongst animals. More rigorous and open-minded inspection (together with a growing body of investigative evidence) does confer that long-standing ‘isolation’ is a violation of natures and life’s preferences.
The queer thing is that there exist recognised rising incidence (trends) of a whole bundle of chronic diseases in the modern human that inhabits the developed world that seem not to afflict other species to the extent they do man. They do not seem to afflict humans that live remote from modern man ans still retain old-world habits of gathering and hunting together with wearing loin cloths and going about business barefoot. Chronic disease in man has both chronological and geographical variations in incidence and the way incidence is trending.
For those who hold high regard for principles of cause and effect (and we all should for the principle of cause and effect is universal) those holistic field based observations should indicate that any increase in effects must arise from increased exposure to ’cause’. Exposure may increase via rises in time (how long exposed), rises in frequency (how often), via increases in intensity (how strong), or even a combination of these.
People and science need(s) to wake up to a stark reality that the rise in incidence of a whole bundle of chronic diseases and conditions of ill-health correlates with the time-line of four major league advances in human technologies.
Electric light, rubber, plastic, and the materials, methods, and fabrics used to construct and furnish the places we live in, work in, and even ‘play’ in, have resulted in a trend from having frequent contact with ground established millions if not billions of years back in the evolution of life to the sate of having next to none at all. Humans now have a dysfunctional relationship with light (seen through the eyes of nature) wrought by the ubiquity and intensity of artificial light which has consequences for a key physiological factor, cortisol, and which has cortisol (levels and circadian patterns) trending to dysfunctional too. Then in turn cortisol’s loss of balance and rhythmic cascades into other physiological factors, perhaps emphasising insulin together with the HPA axis.
One can counter disruption to cortisol by redressing the aberrant ways a person may interact with light (not enough exposure to daylight and/or too much exposure to artificial light) such that the relationship becomes more in tune with natural cycles of day and dark. Intriguingly making it a persons habit to sleep on a bed equipped with an earthing sheet (or taking other purposeful steps to connect to ‘ground’) has (evidence backed) beneficial effects restoring balance and rhythmicity to cortisol secretion and concentrations in the least, insulin arguably, insulin sensitivity, and perhaps ranging to a suite of other physiological factors.
And because I have sound reasons to do so I think the habit of earthing, redressing isolation as it does, positively impacts upon membrane potentials for potentially every cell and every cell-type in the body which in turn has appreciable health benefits for those individual cells (in their trillions) and thus has health benefits for us.
By what standards could we judge a cells health?
After conception be began life a cluster of cells each one indistinguishable from any other. These cells are blessed with pluripotency – the very same phenomenon so revered in stem cells. Those pluripotent cells trended over gestation to to develop into each one of many different cell types needed to make a complete human and did so in all the right places (coordinates) within that cluster. The cluster for limb-buds and began to establish anatomical form. Yet the DNA in every cell remained the same only the coding that applies to DNA (the epigenome) began trending over time. Cell types, the many hundred differentiated cell types needed to make an adult, are differentiated not by the genome but by the epigenome. The integrity of function of a cell type is defined by the integrity of the epigenome and epigenetic differentiation between cell types. Thence corruption of the epigenome specific to a cell or cell type is one way via which integrity of function of that cell or cell type may be degraded and compromised.
Healthy cells do what they should when they should and thus give rise to healthy tissues and healthy organs which thus in turn maintains a healthy ‘us’. So cells cease to be 100% healthy when they cease to do what they should when they should in response to circumstances that come before them (and ‘us’).
There are grounds to concede the possibility that the health of cells is highly dependent (amongst other things) upon optimal membrane potentials.
We do so readily overlook that that the health of us is a function of the health of our cells and the health of their membranes. Membranes are not inert. They exert influence over cell expression. Earthing offers a basket of benefits (for a suite of reasons) and over a bundle of chronic health conditions. OSA is not a bad place to begin with curiosity no matter how sceptic a person is inclined to be.