
Estimated reading time: 11 minutes
Melatonin is a hormone that regulates sleep, wakefulness, and circadian rhythms in humans.
Circadian rhythm describes the sleep/wake cycle, a biological clock that runs in our brain and cycles between sleepiness and alertness. It explains why we may feel energized or sleepy at around the same time each day.

We all know that sleep is crucial for our health and wellbeing. But, sadly, millions of people suffer from sleep disorders. It is believed that about one-third of Americans suffer from some sleep problems.
The most common issues are waking up in the morning feeling drowsy or tired, followed by waking up in the middle of the night, difficulty going back to sleep after waking up and difficulty falling asleep initially (1).
Insomnia is defined as difficulty falling asleep or staying asleep, even when we have the chance to do so. People with insomnia are usually unhappy with their sleep and often experience fatigue, low energy, difficulty concentrating, mood disturbances, and decreased performance in work or at school (2).
Insomnia can be acute (short-term) or chronic (ongoing)(3). Acute insomnia is often caused by situations such as stress at work, family issues or a traumatic event. This type of insomnia may last for days or weeks. Chronic insomnia lasts for a month or longer.
There are several ways to deal with insomnia. Treating a possible underlying cause is usually the first step. This may include avoiding caffeine, tobacco and other stimulants. Alcohol and certain medicines may also disrupt sleep.
Cognitive behavioral therapy may be helpful (4). Such treatment targets thoughts and actions that may disrupt sleep and encourages good sleep habits.
Several medicines are available to treat insomnia, including over-the-counter (non-prescription) and prescription medications. Such sleep aids may cause side effects such as daytime sedation and dizziness, and some are associated with risk of tolerance, dependence, and addiction.
Melatonin is often recommended to treat insomnia. It is available as a food supplement in health food stores. No substantive risks from melatonin use have been reported. However, several questions remain about its efficacy which may depend on drug dose and formulation, as well as the timing, frequency, and duration of administration (5).
1. What Is Melatonin?
Melatonin (N-acetyl-5-methoxy tryptamine) is a hormone produced by the pineal gland in animals and humans.
The pineal gland is a small gland located deep in the center of the brain
Three centuries ago, the French philosopher René Descartes described the pineal gland as “the seat of the soul.” However, it was not until the late 1950s that melatonin was identified (6)
Melatonin is synthesized from the essential amino acid tryptophan.
2. What Foods Contain Tryptophan?
Essential amino acids cannot be made by the body. As a result, they must come from food.
The highest levels of tryptophan are often found in complete proteins like red meat, fish, poultry, milk, and eggs. While most plant sources do not contain as much tryptophan as meat or dairy products, there are many plant-based options available including chickpeas, cashews, cauliflower, kidney beans, and quinoa (7).
Serotonin is a brain neurotransmitter, and an essential biochemical messenger and regulator. The metabolism of tryptophan into serotonin requires nutrients such as vitamin B6, niacin, and glutathione.
3. What Is the Relationship Between Tryptophan, Serotonin, and Melatonin?
The biosynthesis of melatonin is initiated by the uptake of the uptake of tryptophan into the pineal gland.
The cells of the pineal gland convert tryptophan to another amino acid, 5-hydroxytryptophan, through the action of the enzyme tryptophan hydroxylase and then to 5-hydroxytryptamine (serotonin) by the enzyme aromatic amino acid decarboxylase (8).
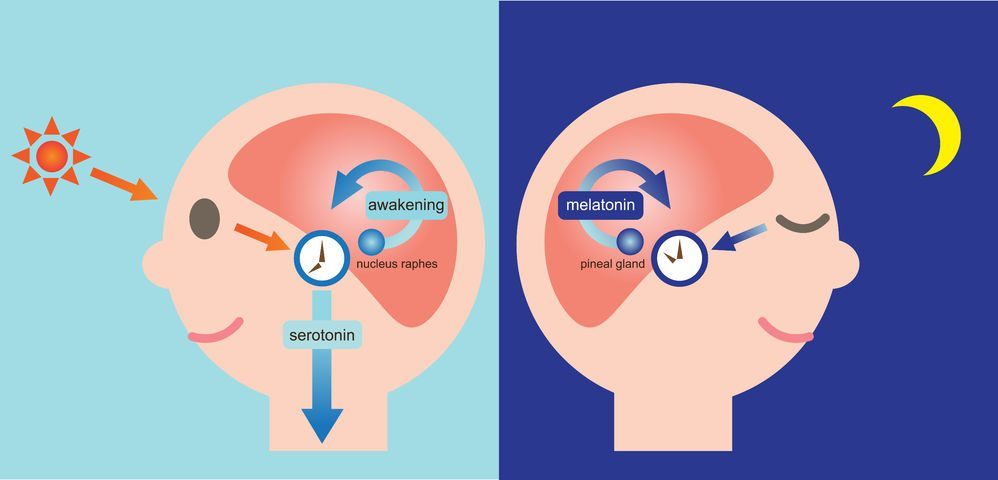
Serotonin concentrations are higher in the pineal than in any other organ or in any brain region. There is a striking diurnal rhythm with serotonin remaining at a maximum level during the daylight hours and falling by more than 80% soon after the onset of darkness as the serotonin is converted to melatonin, 5-hydroxytryptophol and other methoxyindoles (8).
In short:
- Tryptophan is an essential amino acid
- Tryptophan is a precursor for the formation of serotonin and melatonin
- The pineal gland converts tryptophan to serotonin which is then converted to melatonin
- Serotonin levels are maximal during daylight hours
- Serotonin levels drop after the onset of darkness as the pineal gland converts most of the serotonin to melatonin
4. When Does the Pineal Gland Secrete Melatonin?
Melatonin secretion manifests a circadian rhythm. Secretion is low during daylight, ascending after the onset of darkness, peaking in the middle of the night between 11 PM and 3 AM, and then falling sharply before the time of light onset (9).
Interestingly, high nocturnal concentrations of melatonin are characteristic of both diurnally active species (like humans), in which high levels promote sleep, and nocturnally active ones (like rats), in which melatonin has no apparent relationship to sleep (10).
The melatonin produced by the pineal gland diffuses into the cerebrospinal fluid and the bloodstream. Melatonin is highly lipid soluble and diffuses freely across cell membranes. It travels in blood primarily bound to the protein albumin.
5. Is There a Seasonal Variation in Melatonin Concentration?
Melatonin secretion by the pineal gland appears to have a seasonal rhythm. Hence, melatonin levels are higher in the fall and winter and lower in the spring and summer (6).
People with seasonal affective disorder (SAD) typically feel sad or down during the winter months. In some cases, this may develop into a subtype of clinical depression that lasts throughout the late fall and winter months.
Excessive duration of melatonin secretion has been implicated in SAD, but researchers are far from settled on this theory.
Some studies have shown that people with SAD may have increased duration of melatonin secretion in the early morning hours. This would explain why people with SAD have difficulty waking up and don’t feel alert in the morning. Nevertheless, low-dose melatonin taken at night may sometimes be useful in improving mood in patients with SAD (11).
6. Does Age Affect Melatonin Levels?
There is a marked age variation in melatonin secretion by the pineal gland.
Melatonin Secretion starts during the third or four months of life, coincident with sleeping at nighttime becoming more common. It then increases rapidly to peak at ages two and three years, then declines slightly to a plateau that lasts throughout early adulthood (10).
Melatonin secretion declines with advancing age. At the age of 70, nocturnal concentrations are only a quarter or less of what they are in young adults (12).
One rationale for administering supplemental melatonin to older adults with sleep disorders is to compensate for the age-related decline in melatonin secretion.
7. What Are Melatonin Sleep Aid Supplements?
In the United States, melatonin is defined by the US Food and Drug Administration as a dietary supplement. Hence it can be purchased at any dose without a prescription.
In the European Union, melatonin is defined as a prescription drug and is not available over-the-counter. Based on the currently available evidence, 1 mg of melatonin is recommended close to bedtime to reduce sleep onset latency.
Melatonin supplements are available as pills, liquids, and chewable. You may find them in natural or synthetic forms.
Despite claims to the contrary, all of the melatonin sold in the United States is of synthetic origin (10).
As the sale of melatonin is not regulated in the US, very high doses can be sold and may contain additives with potential side effects.
Unlike with many other sleep medications, you are unlikely to become dependent on melatonin, have a diminished response after repeated use (habituation) or experience a hangover effect (13).
8. Is It Scientifically Proven that Melatonin Can Help You Sleep?
Yes, indeed it is. Several studies have shown that melatonin may positively affect several measures of sleep.
A systematic analysis of several placebo-controlled studies showed that melatonin treatment significantly reduced sleep onset latency, increased sleep efficiency, and increased total sleep duration (14).
9. What Doses of Melatonin Should be Used to Promote Sleep?
A dose of 0.1 – 0.3 mg of melatonin before sleep is adequate. This dose will raise the nocturnal plasma concentration of melatonin into the normal range observed in young adults (15).
Although melatonin is generally considered relatively nontoxic, it is worth keeping in mind that some marketed doses, such as 10 mg, can raise plasma concentrations 60 times their normal values (16).
Very high levels of melatonin may be associated with side effects such as daytime sleepiness, tiredness, and hypothermia.
Experts have also suggested that when the melatonin receptors in the brain are exposed to too much of the hormone, they may become unresponsive (17). This would mean that the drug stops doing what it is supposed to do.
10. When Is the Best Time to Take Melatonin?
If you have trouble falling asleep you should take melatonin at night. Taking melatonin 30-60 minutes before you go to sleep is a good option.
People who are night owls and usually go to bed late may want to take melatonin 2-3 hours before the desired bedtime, at least if they want to go to sleep earlier than usual.
11. What Is the “Phase Shift Theory” About?
The circadian rhythm of melatonin production typically reflects our biological clock, sometimes called the circadian pacemaker.
According to the “Phase Shift Theory”, some people may be “phase-advanced,” meaning their bodies release melatonin too early in the evening, while others may be “phase-delayed,” meaning they continue to release melatonin for too long into the day.
A substantial number of studies have shown that the onset of melatonin secretion under dim light conditions (the dim light melatonin onset or DLMO) is the single most accurate marker for assessing the circadian pacemaker (18).
The DLMO has been used to assess whether an individual is entrained (synchronized) to the 24-h light-dark cycle or is free-running, or whether an entrained individual is abnormally phase-advanced or phase-delayed (19).
Phase-advanced individuals have DLMOs that occur abnormally early in the evening, usually between 6 and 8 p.m. Phase-delayed individuals have DLMOs that occur after 10 p.m.
Winter depressives tend to have slightly delayed DLMOs. They also have difficulty waking up in the morning, a clinical finding that is associated with phase-delayed circadian rhythms (20). These people are similar to individuals who have delayed sleep phase syndrome (DSPS). Characteristic of DSPS is difficulty falling asleep before 1 a.m.
People who tire easily in the evening and cannot extend their sleep past 3-5 a.m. often have advanced sleep phase syndrome (ASPS).
12. Can Melatonin Be Used to Phase Shift the Human Circadian Clock?

Air travelers have transient DSPS after flying eastward and transient ASPS after flying westward.
Hence, when traveling eastward, it will be more difficult to fall asleep in the evening and harder to get up in the morning. When going westward, staying awake in the evening will be more difficult and we’ll be likely to wake up early in the morning.
Night workers have ASPS during their work weeks and DSPS on their off-work days.
Melatonin, even when administered at a physiological dose (0-3- 0.5 mg) can shift our circadian phase (21). This could promote the adaptation to air travel and night work.
13. Can Melatonin Be Used To Prevent and Treat Jet Lag?
Melatonin has been widely studied as a jet lag remedy. Melatonin may aid sleep during times when you wouldn’t normally be resting which may be helpful against jet lag.
According to an analysis of Cochrane data, melatonin is remarkably effective in preventing or reducing jet lag, and occasional short-term use appears to be safe (22). It should be recommended to adult travelers flying across five or more time zones, particularly in an easterly direction, and especially if they have experienced jet lag on previous journeys. Travelers crossing 2-4 time zones can also use it if need be.
According to this data, daily doses of melatonin between 0.5 and 5 mg are similarly effective, except that people fall asleep faster and sleep better after 5 mg than 0.5 mg. Doses above 5 mg appear to be no more effective.
The timing of the melatonin dose is important: if it is taken at the wrong time, early in the day, it is liable to cause sleepiness and delay adaptation to local time. The incidence of other side effects is low.
14. Can Melatonin Improve Daytime Sleep In Night-Shift Workers?
There is substantial evidence that the prevalence of sleep disorders is a significant occupational health problem among night shift workers.
Melatonin may be an effective treatment for shift workers with difficulty falling asleep.
One study found that melatonin may improve daytime sleep in night-shift workers (23).
Another study found that 5 mg of melatonin taken 30 minutes before nighttime sleep reduced sleep onset latency among nurses following recovery from night work (24).
15. What Are the Side Effects of Melatonin?
Even though melatonin is an unregulated drug in many countries and is commonly used in excessive doses, adverse effects seem to be relatively uncommon.
Drowsiness, headache, fragmented sleep, dizziness, and nausea are among the side effects that have been described.
It is not known whether melatonin will harm an unborn baby or a nursing infant. Hence, it should be avoided during pregnancy and breastfeeding.
Furthermore, there have been no long-term safety studies of the use of melatonin in children and adolescents.
Also, melatonin supplements can interact with various medications, including anticoagulants and antiplatelet drugs, anticonvulsants, contraceptive drugs, diabetes medications and drugs that suppress the immune system.
“Timed release”, or “sustained release” melatonin!
Gets you to sleep and keeps you asleep through the middle of the night. It’s a seemingly sound idea.
What do you think?
A few clinical trials have addressed prolonged-release melatonin. There appears to be an improvement in sleep quality and latency, and maybe morning alertness as well, compared to placebo. However, there is no direct comparison with short acting melatonin.
https://www.ncbi.nlm.nih.gov/pubmed/23044640
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4319556/
https://www.ncbi.nlm.nih.gov/pubmed/20712869
Thanks, Doc.
For so long it felt as if I’d never sleep well again. I’d given up hope, accepted being an insomniac and that I’d always be tired and irritable through the day. It wasn’t until I found this natural program to cure insomnia ( fallasleep-instantly.bestips.info ). I’m now falling asleep fast for at least 6 hours straight, and I no longer need coffee to prop me up through the day.
Type of light is also important for the circadian cycle. The eye has sensors that monitor the amount of blue and turquoise wavelengths of light. Large amounts inhibit melatonin and create alertness. A lack of this color light signals the body to create melatonin and relaxation. An hour before bed, the only light I use is an SCS Sleep Ready Light Blub, which doesn’t have those wavelengths. Programs like f.lux for computers block blue light at night. Cell phones usually have this feature, or it can be found as an app. To promote energy upon awakening, let light shine through the windows, or use a lightbulb with a high color temperature like 5000K to tune down the melatonin and kick up the energy. Also, an hour before bed, I avoid cell phone use and television which are very stimulating. Low color lightbulbs like 2700K or 3000K in bedrooms are a relaxing light.
Awesome blogg. thanks
I generally refer to https://www.dealsshutter.com/medlife-coupons for tips and news.
I have had chronic nerve issues and insomnia for months now and blood pressure very high on agitation and normal while hospitalised.Last night I took 10mg Melatonin and B6 which had me sleep all night and feel much better on rising.Gradually over the day I walked well and blood pressure was normal so wonder if it is all right to take another tonight as I still feel jittery without high be..Sorry bit confused any help here ?