
Emotional stress is a known risk factor for developing heart disease (1). Never is this relationship more evident than in the broken heart syndrome, an acute heart disorder that is directly precipitated and caused by an emotionally stressful event.

The broken heart syndrome, also called stress cardiomyopathy (stress-induced cardiomyopathy), apical ballooning syndrome, or takotsubo cardiomyopathy was first described 1990 in Japan (2). Although its symptoms mimic those of an acute heart attack, it is a completely different disorder and is not caused by blocked coronary arteries.
Patients with stress cardiomyopathy experience sudden, intense chest pain precipitated by an emotionally stressful event. It could be the death of a loved one, breakup of a relationship, domestic abuse, arguments, devastating financial losses or a natural disaster.
The Broken Heart Syndrome (Stress Cardiomyopathy) – The Basics
In stress cardiomyopathy, a part of the heart muscle loses its pumping capacity while the rest of the heart pumps normally or with more forceful contractions. A severely reduced contraction of the apex of the left ventricle of the heart is typical.
Although the initial symptoms may be severe, stress cardiomyopathy is a reversible disorder, and normal left ventricular function is usually restored within a few weeks.
Takutsubo
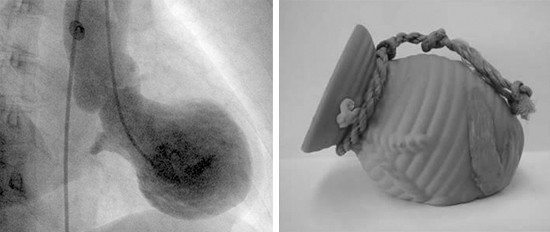
The term “takotsubo” is a name for a Japanese octopus fishing pot that has a specific shape (a narrow neck above a wider portion) that is similar to the ballooning configuration of the left ventricle of the heart usually seen in patients with stress cardiomyopathy.
Typically, the contraction of the mid- and apical segments of the left ventricle are depressed, and there is increased contraction of the proximal part (basal segment), creating a balloon-like appearance when the heart muscle contracts. Less common variants include depressed contraction of other segments of the left ventricle creating a somewhat different picture (3).
Acute Coronary Syndrome and the Broken Heart Syndrome (Stress Cardiomyopathy)
The clinical presentation of stress cardiomyopathy is very similar to that of an acute coronary event. Therefore, patients with stress cardiomyopathy are usually admitted to the coronary care unit (CCU) for observation, further workup and treatment.
Acute coronary syndrome (ACS) is the most common reason for admission to the CCU.
ACS usually presents as sudden chest pain accompanied by typical changes in the electrocardiogram (ECG) and/or elevation of cardiac markers, such as troponin T in blood. The majority of ACSs are caused by reduced blood flow in a coronary artery caused by atherosclerosis and clot formation at the site of atherosclerotic plaque.
If a part of the heart muscle suffers irreversible damage due to lack of blood flow, the situation is defined as acute myocardial infarction (acute heart attack).
Although myocardial infarction and stress cardiomyopathy have many similar features, the latter is not caused by a blocked coronary artery.
Approximately 1.7 to 2.2 percent of patients admitted for ACS have stress cardiomyopathy (4).
Although stress cardiomyopathy is not caused by an arterial blockage, it can occur in patients with coexisting coronary artery disease.
What Is the Underlying Cause of The Broken Heart Syndrome (Stress Cardiomyopathy)?
The underlying pathophysiology of stress cardiomyopathy is not well understood.
The disorder is more common among women than men and is most common among postmenopausal women.
Although the clinical presentation is similar to that of acute myocardial infarction (acute heart attack), coronary angiography typically shows an absence of blockages of the coronary arteries unless there is coexisting coronary artery disease.
As the onset of the disorder is usually, but not always triggered by an acute medical illness or intense emotional stress, it has been postulated that catecholamine excess plays an important role. Catecholamines are hormones produced by the adrenal glands and usually released into the blood when a person is under physical or emotional stress. The main catecholamines are dopamine, norepinephrine, and epinephrine (adrenalin).
Catecholamines can cause arterial spasm and microvascular dysfunction, possibly resulting in stunning of a portion of the left ventricle (5). Furthermore, catecholamines may have direct toxic effects on heart muscle cells (6).
A key role of catecholamines in stress cardiomyopathy is supported by studies showing significantly higher levels of catecholamines in patients with stress cardiomyopathy compared to those with myocardial infarction resulting from a blockage of a coronary artery (7). However, elevated catecholamines are not always present, and some studies have reported normal levels (8).
Symptoms, Diagnosis and Complications
The clinical symptoms of stress cardiomyopathy are similar to that of acute myocardial infarction. Central chest pain is the most common complaint, but some patients present with breathlessness, syncope (fainting) or shock.
Stress cardiomyopathy can easily be misdiagnosed as myocardial infarction because symptoms and test results are very similar.
The Mayo Clinic has proposed the following criteria for the diagnosis of stress cardiomyopathy (9). All four criteria are required for the diagnosis.
- Transiently reduced contraction of left ventricular mid segments with or without apical involvement. The wall motion abnormalities typically extend beyond a that supplied by a single coronary artery. A stressful trigger is often, but not always, present.
- Absence of obstructive coronary disease or angiographic evidence of acute plaque rupture.
- New ECG abnormalities (either ST-segment elevation and/or T-wave inversion) or modest elevation in cardiac troponin.
- Absence of pheochromocytoma or myocarditis.
Patients with stress cardiomyopathy will usually undergo similar workup as patients with myocardial infarction. Repeated blood samples and ECGs are performed. Echocardiography is used to assess the contraction of the left ventricle and the state of the heart valves.

Coronary angiography, a specific imaging technique to visualise the coronary arteries, is performed to study blood flow in the coronary arteries and to assess whether blockages are present or not.
Stress cardiomyopathy may cause irregular heart rhythm (arrhythmia), the most serious being ventricular tachycardia or ventricular fibrillation. Pulmonary edema and shock may also occur.
In severe cases, stress cardiomyopathy may lead to shock with low blood pressure and decreased urine output.
Treatment and Prognosis
Although patients with stress cardiomyopathy may become critically ill during the initial phase, it is a transient disorder. There is no curative treatment and patients are managed with supportive therapy. Resolution of the initial physical or emotional stress that provoked the disorder usually results in rapid resolution of symptoms.
Treatment is based on the patient’s overall condition. Diuretics, angiotensin-converting enzyme inhibitors, and beta blockers are often admitted to treating heart failure, left ventricular dysfunction or tachycardia. If atherosclerosis is present, aspirin and statins are recommended.
Echocardiography (ultrasound of the heart) may reveal a blood clot (thrombus) within the left ventricle in which case anticoagulation (blood thinners) should be administered.
Although left ventricular function may be severely affected during the initial phase, recovery is usually complete. Normal left ventricular function is usually restored within one to four weeks (10).
Reported in-hospital mortality is approximately 2 percent (11). A follow-up study that lasted 4.5 years showed that recurrence may occur in approximately 10 percent of cases (12).
Typo under this heading:
What Is the Underlying Cause of Stress Cardiomyopathy?
I believe you meant to say “than” in this sentence. “The disorder is more common among women “and” men and is most common among postmenopausal women.”
Thanks David. Appreciate it. It’s been corrected.
I relate totally to this, having experienced it. I was in a religious cult and thought i was going to die.