
Cardiovascular imaging has revolutionized the assessment of heart disease, providing powerful tools to detect and evaluate coronary artery disease (CAD) before it leads to serious complications.
Two common heart imaging tests—CT Calcium Scoring (CAC) and CT Coronary Angiography (CCTA)—serve distinct purposes. While both utilize computed tomography (CT) technology, they differ significantly in what they measure, their indications, and their clinical implications. Understanding these differences is crucial for both healthcare professionals and individuals seeking to optimize their heart health.
CT Calcium Score: Measuring the “Silent” Risk
What It Measures
CT Calcium Scoring quantifies the amount of calcified plaque in the coronary arteries as described in another article on this blog (1). It does not visualize soft plaque or assess coronary artery narrowing directly. Instead, it provides an Agatston score, a numerical representation of coronary calcium burden.
Why Is It useful?
Calcium deposits in the coronary arteries indicate the presence of atherosclerosis, a key contributor to heart disease. Since coronary calcium is an objective marker of lifetime exposure to risk factors (such as high LDL – cholesterol, high blood pressure, and smoking), CAC scoring is a powerful tool for risk stratification.
Who Should Consider It?
- Asymptomatic individuals with intermediate risk of CAD (based on factors like age, cholesterol levels, and family history).
- Those uncertain about whether they should start statin therapy.
- Individuals looking for a refined cardiovascular risk assessment beyond traditional cholesterol or blood pressure measurements.
How the Score is Interpreted
- 0: No detectable calcium, very low risk of coronary heart disease.
- 1-99: Mild evidence of coronary artery disease, low-to-moderate risk.
- 100-399: Moderate plaque burden, increased risk of a future cardiovascular event.
- 400+: High risk of significant coronary artery disease and potential future heart attacks.
Impact of Age and Gender
Interpreting Coronary Artery Calcium (CAC) scores requires consideration of age and gender, as both factors significantly influence calcium deposition in coronary arteries.
Studies have demonstrated that the prevalence and extent of coronary artery calcification increase with age and are generally higher in men compared to women of the same age group. For instance, research indicates that a non-zero CAC score corresponds to the high-risk category in women under 55 years and men under 45 years.
Therefore, a CAC score of 100 suggests a higher risk in a 40-year-old than in a 70-year-old. Additionally, women tend to develop calcified plaques later in life compared to men, implying that a given CAC score may represent a different level of risk between genders.
These variations underscore the importance of interpreting CAC scores within the context of an individual’s age and gender to accurately assess cardiovascular risk (2).
Limitations
- It does not assess the degree of coronary artery blockage or detect soft (non-calcified) plaque.
- A score of zero does not completely rule out the presence of non-calcified plaques or future heart disease.

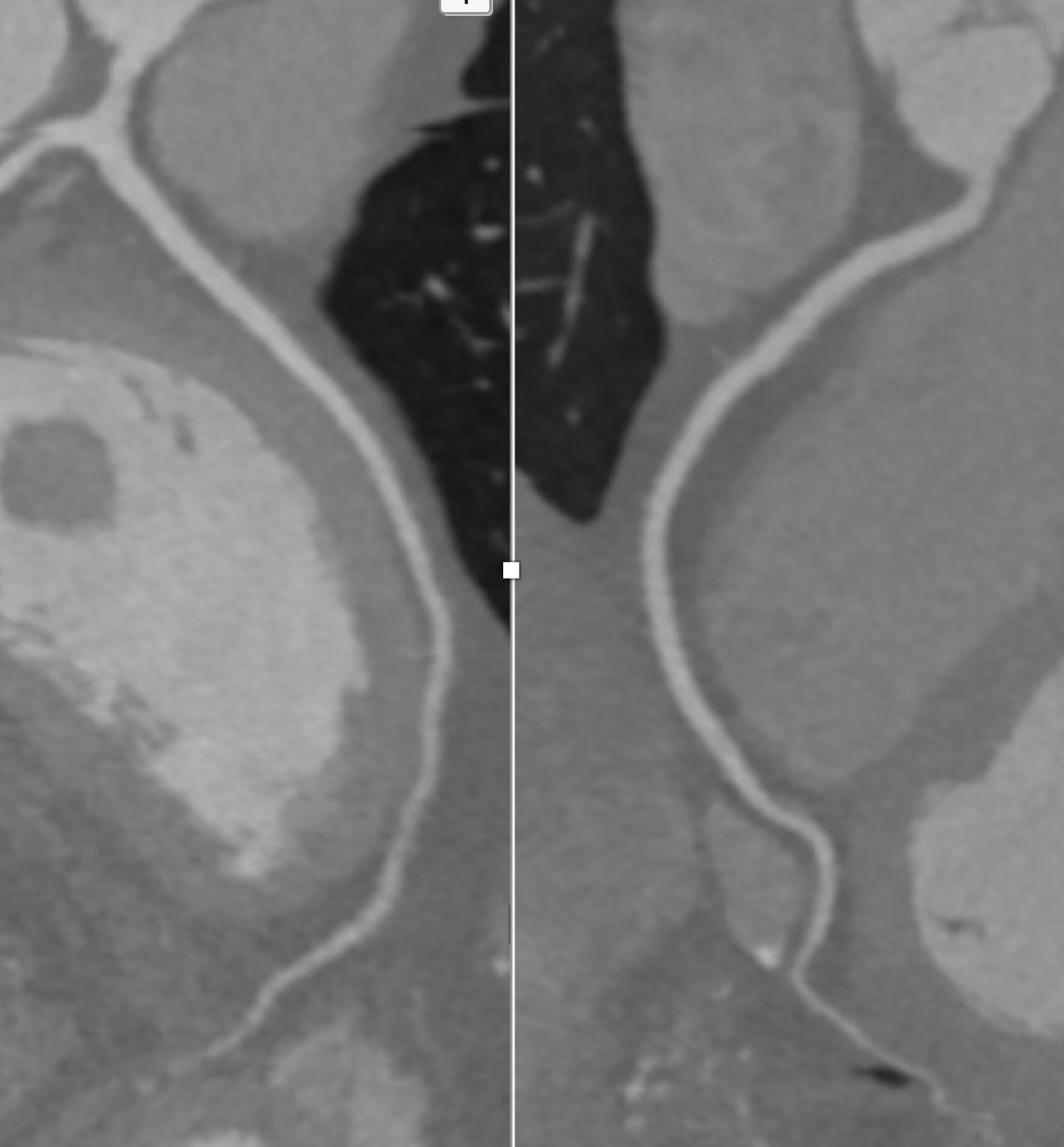
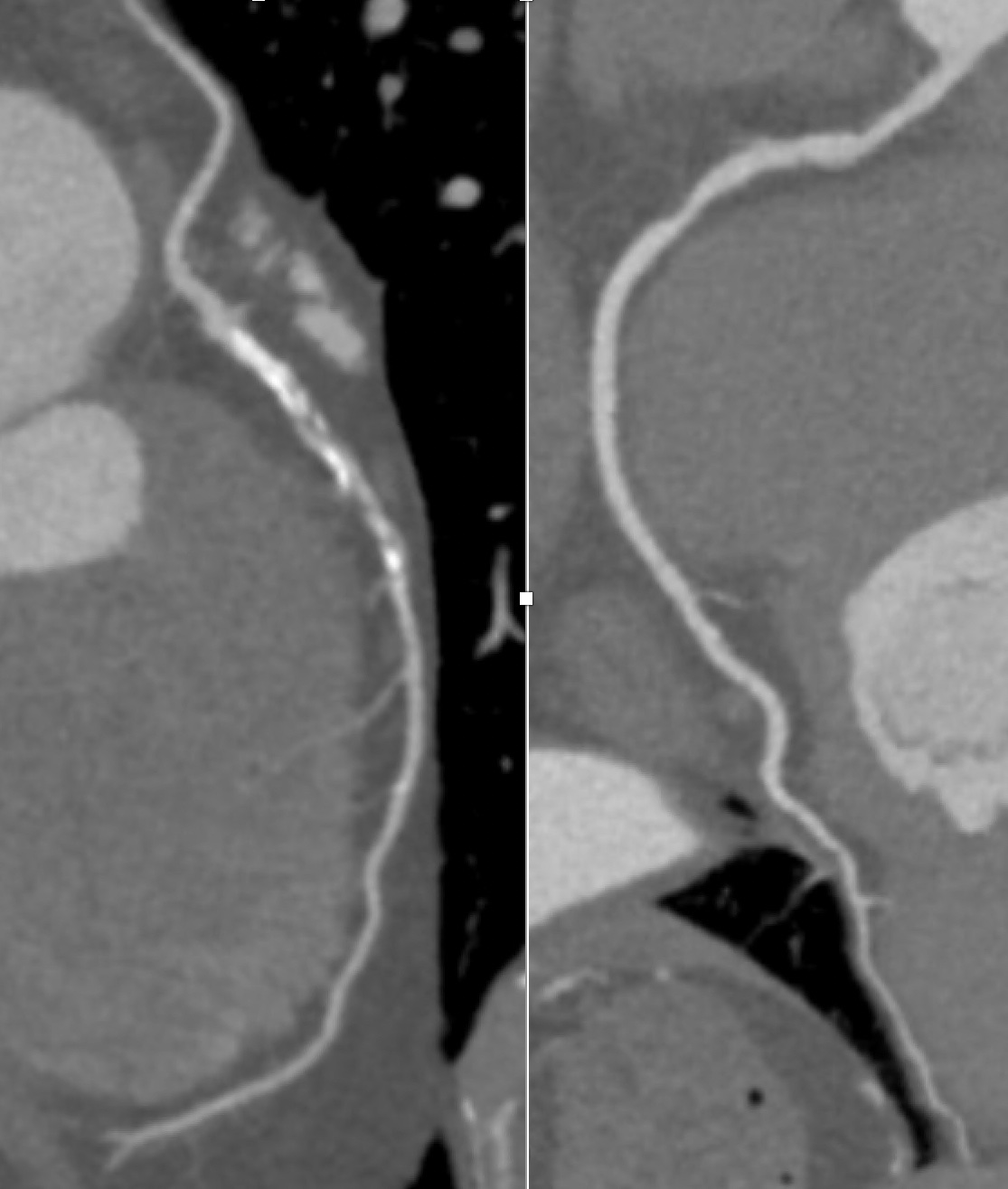
CT Coronary Angiography. Left: Left anterior descending (LAD) coronary artery with mixed plaque (both calcium and soft plaque). Right: Right Coronary Artery (RCA) with soft plaque in proximal part and mild to moderate stenosis.
CT Coronary Angiography: Seeing the Whole Picture
What It Measures
CT Coronary Angiography (CCTA) provides a detailed visualization of both calcified and non-calcified plaques, as well as the degree of narrowing (stenosis) in the coronary arteries. It involves injecting contrast dye into a vein to enhance the imaging of blood flow through the coronary arteries.
Why Is It useful?
CCTA is an anatomic imaging modality that visualizes coronary artery structure, plaque burden, and stenosis severity. It can be particularly valuable in evaluating chest pain and identifying early signs of obstructive coronary artery disease before symptoms become severe.
Who Should Consider It?
- Patients with chest pain but no history of prior heart disease.
- Individuals with equivocal stress test results.
- Those with suspected anomalous coronary arteries (anatomic variations that may impact blood flow).
- Patients with a high CAC score who need further assessment of plaque burden and stenosis severity.
How the Results are Interpreted:
- No significant stenosis: Less than 50% narrowing, low likelihood of obstructive CAD.
- Moderate stenosis: 50-70% narrowing, may require further evaluation with stress testing or invasive angiography.
- Severe stenosis: Greater than 70% narrowing, often indicates the need for intervention such as stenting or bypass surgery.
Limitations
- Requires IV contrast and radiation exposure (though lower than conventional catheter-based angiography).
- May yield false positives due to motion artifacts or heavily calcified arteries, leading to unnecessary follow-up testing.
- Less useful for individuals with extensive coronary calcification, where calcium “blooming” can obscure critical stenoses.
Key Differences – A Quick Comparison
|
Feature |
CT Calcium Score (CAC) | CT Coronary Angiography (CCTA) |
|---|---|---|
| Purpose | Risk assessment | Diagnosis of CAD |
| Visualizes Soft Plaques? | No | Yes |
| Assesses Blockages? | No | Yes |
| Contrast Dye Needed? | No | Yes |
| Radiation Exposure | Low | Higher |
| Best For | Asymptomatic risk stratification | Symptomatic CAD evaluation |
What Do the Most Recent Guidelines Say?
The 2024 European Society of Cardiology (ESC) Guidelines for the Management of Chronic Coronary Syndromes (CCS) provide updated recommendations on the use of Coronary Artery Calcium (CAC) scoring and Coronary Computed Tomography Angiography (CCTA) in diagnosing and managing chronic coronary artery disease (3).
The latest European guidelines recommend CT Calcium Scoring (CAC) for people without symptoms who have a low to moderate chance of heart disease. If the score is zero, their risk is very low, meaning they may not need further testing. CT Coronary Angiography (CCTA) is preferred for people with chest pain or other heart symptoms, as it provides a detailed image of the arteries to check for blockages. If doctors suspect a high risk of heart disease, they may recommend additional tests, like stress imaging, to see how well the heart is working.
The 2023 AHA/ACC guidelines recommend CT Calcium Scoring (CAC) to assess heart disease risk in people without symptoms, with a score of zero indicating very low risk. CT Coronary Angiography (CCTA) is advised for those with chest pain or suspected coronary artery disease, as it provides detailed images of artery blockages. These tests should be used based on a person’s risk factors and symptoms, helping doctors decide on the best approach for prevention or treatment (4).
Hence, according to recent guidelines, CCTA is increasingly recommended as a first-line test for stable chest pain, often preferred over traditional stress tests when evaluating suspected coronary artery disease.
Which Test is Right for You?
Both CT Calcium Scoring and CT Coronary Angiography have important roles in cardiovascular risk assessment and disease detection. CAC scoring is best for predicting long-term risk and guiding preventive strategies, while CCTA is more appropriate for evaluating active symptoms and diagnosing coronary artery disease.
For individuals at intermediate risk of heart disease but with no symptoms, a calcium score can provide clarity on whether preventive measures (such as statin therapy) are necessary. On the other hand, for those with concerning symptoms such as chest pain, CCTA is the superior choice for identifying obstructive plaques and ruling out significant coronary blockages.
Ultimately, the decision on which test to undergo should be made in consultation with a physician, considering an individual’s risk factors, symptoms, and overall cardiovascular profile.
The Bottom Line
The evolution of cardiac imaging has provided clinicians with incredible tools to assess coronary artery disease at various stages. Understanding the differences between CT Calcium Score and CT Coronary Angiography empowers both patients and healthcare providers to make informed decisions regarding cardiovascular health.
While these tests are not interchangeable, they complement each other—CAC for long-term risk assessment, and CCTA for diagnosing active coronary disease. As always, lifestyle modifications and preventive measures remain the foundation of heart health, but advanced imaging can provide crucial insights that guide effective treatment strategies.
If you’re considering one of these tests, consult with your doctor to determine the most appropriate choice based on your risk factors and symptoms.
Portions of this article were developed with the assistance of ChatGPT, an AI language model by OpenAI, to help refine structure, language, and clarity while preserving the author’s voice and scientific integrity