
In the early fall of 1975, two mothers from Old Lyme, Connecticut, desperately sought medical help because of a mysterious outbreak of a strange, unexplainable disease. Both children and adults were affected, and arthritis appeared to be the most prominent symptom.
It was soon discovered that many patients also reported a skin lesion with an expanding bulls-eye pattern a few weeks preceding the onset of arthritis (1).
The lesion matched the description of erythema migrans, a skin lesion previously reported in Europe and thought to be a result of an infectious agent. However, this was the first time erythema migrans had been associated with arthritis (2).

In December 1975, a surveillance study was carried out in Lyme and surrounding towns on the eastern bank of the Connecticut River. The study was led by Allan C. Steere, MD, and Stephen E. Malawista, MD, from the Rheumatology section of the Yale School of Medicine.
In 1976, Steere and Malawista suggested that Lyme arthritis was a tick-borne disease. They published evidence showing that the incidence of the disorder was 30 times greater on the east side of the river, where Lyme is located than it was on the west side, similar to the difference in deer and deer tick distribution in the area (3).
Scientists later confirmed that ticks indeed are the transmission vector of the infectious agent in Lyme disease.
The risk of Lyme disease is year round, but the highest risk window is late spring into early summer.
Over 300,000 new cases of Lyme disease are estimated to occur every year in the United States (4). Today, Lyme disease is the most common tick-borne disease in the United States, Canada, and Europe.
Fortunately, Lyme disease is rarely life-threatening.
1. What Is the Cause of Lyme Disease?
Lyme disease is caused by a few different species of the spirochete Borrelia.
Spirochetes are long and slender cork-screw-like bacteria, usually only a fraction of a micron in diameter but 5 to 250 microns long. They are tightly coiled and look like small springs or telephone cords (5).
In North America, Lyme disease is caused primarily by Borrelia burgdorferi (6). In Europe and Asia, infections caused by Borrelia afzelii, and Borrelia garinii are more common.

In the northeastern United States, rodents such as the white-footed mouse are the primary reservoir of the Borrelia species.
The spirochetal infection is transmitted by the bite of infected ticks
The risk of exposure to ticks is highest in the woods and the edge area between lawns and woods. Ticks may also be carried by animals and pets onto parks and gardens and into houses. Campers, hikers, and outdoor workers may be exposed in wooded, brushy, and grassy places.
2. How Do Ticks Transmit Lyme Disease?
The spirochetal infection causing Lyme disease is transmitted by the bite of infected ticks of the Ixodes ricinus complex.
There is no evidence that Lyme disease is transmitted from person-to-person through touching, kissing, having sex or sharing silverware or glasses with a person with Lyme disease.
The three tick species that commonly bite people in the eastern United States include the blacklegged tick, the Lone Star tick, and the American dog tick. The blacklegged tick is the only one that transmits Lyme disease in the United States (7).
The blacklegged tick (or deer tick, Ixodes scapularis) spreads the disease in the northeastern, mid-Atlantic, and north-central United States, and the western blacklegged tick (Ixodes pacificus) spreads the disease on the Pacific Coast.
It is believed that ticks need to be attached for 36 to 48 hours before they can transmit Lyme disease bacteria.

Most humans are infected through the bites of immature ticks called nymphs. Nymphs are tiny and often difficult to see. Adult ticks also transmit Lyme disease bacteria, but they are much larger and are more likely to be discovered before they have had time to transfer the bacteria (8).
Ticks obtain blood by inserting their mouth parts into the skin of a person or animal. Ixodes ticks are slow feeders, and one meal can take several days. As they feed, their bodies slowly enlarge.
3. In What Areas Is Lyme Disease Most Common?
For Lyme disease to exist in an area, three environmental elements must be present (8):
- animals that are infected with Lyme disease bacteria
- ticks that can transmit the bacteria, and
- animal hosts (such as mice and deer) that can provide food for the ticks in their various life stages
Lyme Disease is present in North America, Europe, and Asia.
Travelers involved in outdoor activities in forested areas are at risk, including campers, hikers, and hunters. Brushing against vegetation or walking in city parks known to have infected ticks can also put a person at risk.
Risk of Lyme Disease increases during the warmer months when ticks are most active. However, ticks can be found year-round in areas where temperatures are above freezing.
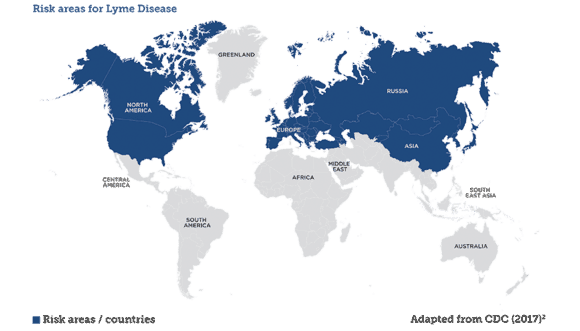 Lyme disease is distributed over a wide geographic area in northern temperate regions of the world.
Lyme disease is distributed over a wide geographic area in northern temperate regions of the world.
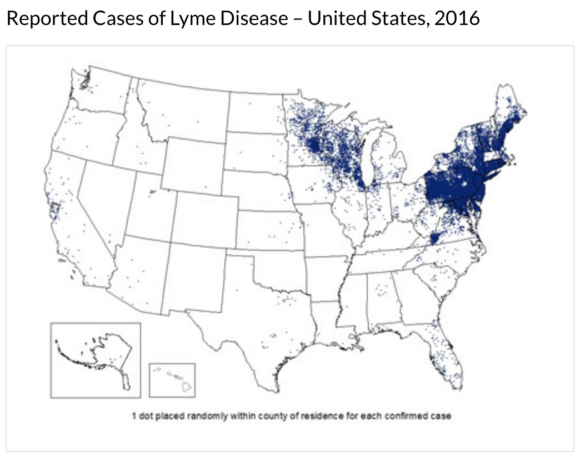
In the United States, most infections occur in the following areas (8):
- Northeast, from Virginia to Maine
- North-central states, mostly in Wisconsin and Minnesota
- West Coast, mainly northern California
4. What Are the Symptoms of Lyme Disease?
The signs and symptoms of Lyme disease are often divided into three clinical stages. However, the clinical features may overlap and some patients present at a later stage with no history of prior signs of the disease (7).
The first stage is characterized by the occurrence of the red, circular, bulls-eye rash called erythema migrans.
The second stage sometimes called early disseminated disease, is characterized by multiple erythema migrans lesions that occur days to weeks following the tick bite. During this period neurological symptoms may occur, including numbness, pain, nerve paralysis, and meningitis (fever, stiff neck, and severe headache). Although rare, some patients experience cardiac involvement including an irregular heartbeat.
The most common clinical manifestations include fatigue, anorexia, headache, neck stiffness, muscle aches (myalgia), joint pain (arthralgias), enlarged lymph nodes, and fever (6).
It is important to acknowledge that different people exhibit different signs and symptoms of Lyme disease. Some patients never develop erythema migrans, some only develop arthritis, and some patients only have neurological symptoms.
General symptoms such as fever, muscle aches, and fatigue can be mistaken for viral infections such as influenza. Joint pain can be mistaken for other types of arthritis, and neurologic signs may be similar to those experienced by patients with multiple sclerosis or peripheral neuropathy of another origin.
The third stage, late Lyme disease is characterized by arthritis involving one or more large joints, especially the knee. Late Lyme disease may occur months to few years following the tick bite and is not always preceded by a history of early localized or disseminated disease.
Neuropsychiatric manifestations may be present during late Lyme Disease. These may include cognitive disturbances and polyneuropathy. The latter is characterized by pain and paresthesias (9).
In Europe, some patients develop a chronic skin condition called acrodermatitis chronica atrophicans (10). It may appear months to years after the initial infection and is mainly due to Borrelia afzelli. The condition is not known to occur in the United States.
5. What Is Erythema Migrans?
The first stage of Lyme Disease, early localized disease, is characterized by a skin lesion called erythema migrans.
Erythema migrans is a red circular rash that often appears at the site of the tick bite. It usually occurs within a month following the bite, most often within the first 3 to 14 days.
Erythema migrans occurs in 80% of patients with Lyme disease (11).
The rash typically expands slowly over the course of days or weeks. Sometimes many rashes appear, varying in shapes and sizes. They are often found on the thighs, groin, trunk, and armpits.
The center of the rash may clear as it enlarges, resulting in a “bulls-eye” appearance. Although the central clearing is classic for erythema migrans, it is usually not present during the first days of the rash.
Erythema migrans is not particularly painful but may occasionally burn or itch and is usually hot to the touch.
Not all rashes that occur at the site of a tick bite are due to Lyme disease. An allergic reaction to tick saliva can also occur and be confused with the rash of Lyme disease. It most often appears within hours to a few days after the tick bite, usually, do not expand, and disappear within a few days.

6. What Are Post-Lyme Disease Syndrome and Post-Treatment Lyme Disease Syndrome (PTLDS)?
The terms pos”post-Lyme disease syndrome” and post-treatment Lyme Disease Syndrome (PTLDS) are sometimes used to describe general symptoms that may be present for long periods after Lyme disease has been treated.
Examples of such symptoms are headache, fatigue, joint pain (arthralgias), musculoskeletal pain, and cognitive difficulties. In most cases, these symptoms disappear gradually in six to twelve months.
Between 5-15 percent of patients treated for Lyme disease may develop PTLDS. The cause of the disorder is unclear but is not believed to be due to persistent or ongoing infection following treatment.
7. What Is Neuroborreliosis?
The term Neuroborreliosis or Lyme neuroborreliosis (LNB) is sometimes used to describe the neurologic manifestations of Lyme disease (12).
Neuroborreliosis may occur during the early and late stages of Lyme disease.
The nervous system is involved in 10% to 15% of cases early Lyme disease (13)
Early neuroborreliosis may present with facial palsy (inability to control the facial muscles on the affected side of the face), meningitis and painful radiculoneuritis (inflammation of one or more roots of the spinal nerves). It usually occurs within about six to twelve weeks following the infection.
The symptoms of acute neuroborreliosis usually disappear following antibiotic treatment.
Late/chronic Lyme neuroborreliosis is characterized by various neuropsychiatric manifestations (14).
The clinical symptoms include seizures, speech difficulties, ataxia (lack of control of voluntary muscle movements), chronic spastic para- tetra- and hemiparesis, mood disorders, psychosis, visual and auditory hallucinations, paranoia, anorexia nervosa, and obsessive-compulsive disorder (15).
8. What Diseases May Resemble Lyme Disease?
Known as “The Great Imitator,” Lyme disease may mimic many other conditions. This may lead to several difficulties in diagnosis.
Muscle aches, fever, and headache are common symptoms of flu. These are also experienced by many patients with Lyme disease.
Arthritis, a common symptom of Lyme Disease, may have many other causes. It may be mistaken for rheumatoid arthritis, gout, osteoarthritis or degenerative arthritis.
Some patients with Lyme disease suffer from chronic fatigue. This may be mistaken for chronic fatigue syndrome or fibromyalgia.
The neuropsychiatric symptoms of Lyme disease may mimic Parkinson’s disease, multiple sclerosis, Alzheimer’s and depression.
9. How Is Lyme Disease Diagnosed?
The diagnosis of Lyme disease should take into account the patients history and exposure to ticks in areas where Lyme disease is known to occur. Hence, detailed travel and activity history is essential.
The diagnosis of early Lyme disease is made on clinical grounds, primarily based on the presence of erythema migrans. Lab tests are unlikely to support the diagnosis at this stage because the immune system will not have had enough time to produce antibodies.
During early disseminated disease and late Lyme disease, lab testing plays a vital role. For serologic testing, a two-tier conditional strategy is recommended (16):
- Enzyme-linked immunosorbent assay (ELISA) test is used most often to detect Lyme disease and detects antibodies to Borrelia burgdorferi. A different type of enzyme immunoassay (immunofluorescent assay or IFA) may be substituted for the ELISA test. However, both these tests can sometimes provide false positive results and are therefore not used as the sole base for diagnosis.
- If the ELISA test is positive, the Western blot test is usually done to confirm the diagnosis.
A negative Western blot test supersedes the result of a positive ELISA or IFA, and testing should be considered negative. A positive Western blot test is considered evidence of an encounter with Borrelia burgdorferi (16).
10. How Is Lyme Disease Treated?
Several antibiotics are useful for treating Lyme disease. These are usually given by mouth but may be given intravenously in more severe cases.
Patients treated with antibiotics in the early stages of the infection usually recover rapidly and completely.
Most patients who are treated in later stages of the disease also respond well to antibiotics.
A few patients may have persistent or recurrent symptoms and may require an additional course of antibiotic treatment. Longer courses of antibiotics have not been shown to be beneficial in patients who have been previously treated and have chronic symptoms.
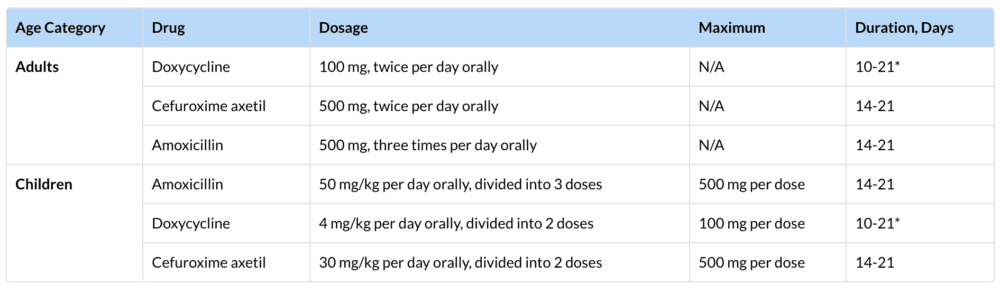
Antibiotics commonly used for oral treatment include doxycycline, amoxicillin, or cefuroxime axetil. People with specific neurological or cardiac forms of illness may require intravenous treatment with antibiotics such as ceftriaxone or penicillin (17).
11. How Is Lyme Disease During Pregnancy Treated?
Untreated Lyme disease during pregnancy may lead to infection of the placenta and possible stillbirth. However, no severe effects on the fetus have been found in cases where the mother receives appropriate antibiotic treatment for her Lyme disease (18).
In general, treatment for pregnant women with Lyme disease is similar to that of non-pregnant adults, although certain antibiotics, such as doxycycline, are not used because they can affect fetal development.
Additionally, there are no reports of Lyme disease transmission from breast milk.
12. How Can Tick Bites Be Prevented?
It is possible to decrease the chances of being bitten by a tick with a few precautions. Avoiding tick-infested areas is the first rule. This is especially important in May, June, and July.
If you live in a risk area, keeping your lawn well manicured and adding a deer fence may be helpful. Because ticks get Lyme disease from mice, eliminating the mouse habitats around your yard is important. This includes removing wood piles and rock piles where the mice tend to live and breed (4).
During outdoor activity, it is important to avoid wooded, overgrown areas and stay out of tall grass and the uncleared regions of the forest. Staying on marked trails is recommended when hiking.
Wearing protective clothing is recommended. That includes long sleeves, long pants and avoid going barefoot or wearing open shoes.
Insect repellant containing DEET, picaridin, IR3535, oil of lemon eucalyptus, para-menthane-diol, or 2-undecanone may be used on the body and Permethrin on clothes. It is imperative always to follow the manufacturer’s instructions when applying these substances.
Permethrin should not be applied to your skin. It is a unique substance and does not need to be reapplied frequently because it stays bound to clothes for several months.
It is a good protective habit to shower immediately or within two hours of coming indoors.
Always check for ticks after being outdoors. Ticks are tiny and sometimes hard to see. By feeling for ticks, they may be found in hidden areas, such as behind your knee or in your armpit.
13. How Should Attached Ticks Be Removed From the Skin?
Because ticks must usually be attached for at least a 24 hours before they can transmit the spirochetes causing Lyme disease, early removal reduces the risk of infection.
The quickest way to remove a tick is with tweezers. Grasp the tick between the head of the tick and the skin and to pull softly but securely away.
Sometimes, parts of the mouth of the tick will be left in the skin. However, these small mouthparts do not transmit Lyme disease and should be left alone. Just leave them in place. They will work their way out on their own.

14. Is a Lyme Disease Vaccine Available?
LYMErix, a vaccine for Lyme disease, received licensing and approval from the U.S. Food and Drug Administration (FDA) in 1998, but the manufacturers (GlaxoSmithKline — then called SmithKline Beecham) stopped selling it in 2002, due to a lack of demand.
The vaccine was based on a specific part of B. burgdorferi called outer surface protein A (OspA). It was found to be between 49 and 68 percent effective in preventing Lyme disease after two injections, and 76 to 92 percent effective in preventing Lyme disease after three injections
In April 2002, GSK announced that even with the incidence of Lyme disease continuing to rise, sales for LYMErix declined from about 1.5 million doses in 1999 to a projected 10,000 doses in 2002. Although studies conducted by FDA failed to reveal that any reported adverse events were vaccine-associated, GSK discontinued manufacturing the vaccine (19). Since then, a new vaccine has yet to appear on the market.
15. Do Ticks Transmit Other Diseases than Lyme Disease?
Lyme disease is the most common tickborne disease in the United States, Canada, and Europe. However, ticks may carry several other diseases than Lyme disease.
Examples of tickborne diseases in the United States are (20):
- Anaplasmosis
- Babesiosis
- Borrelia miyamotoi Disease
- Colorado Tick Fever
- Ehrlichiosis
- Heartland and Bourbon Virus Diseases
- Powassan Virus Disease
- Rocky Mountain Spotted Fever
- Rickettsia parkeri Rickettsiosis
- Tickborne Relapsing Fever
- Tularemia
Examples of tickborne diseases found in other countries are (21)
- African Tick Bite Fever (ATBF, found in Sub-Saharan Africa, Caribbean (French West Indies), and Oceania)
- Tickborne Encephalitis (TBE, endemic in focal areas of Europe and Asia, extending from eastern France to northern Japan and from northern Russia to Albania)
- Mediterranean spotted fever (also known as boutonneuse fever (found in Europe (Mediterranean basin), Middle East, Indian subcontinent,
and Africa) - Crimean-Congo hemorrhagic fever /found in Asia, Africa, and Europe).
- Omsk hemorrhagic fever (found in Southwestern Russia)
- Kyasanur Forest disease (found in Southern India, Saudi Arabia (aka Alkhurma disease in Saudi
Arabia).