
Estimated reading time: 4 minutes
A hugely important question for the clinical cardiologist is whether Covid-19 vaccinations reduce the risk of cardiovascular complications following Covid-19 infections.
It is well-documented that being infected with SARS-CoV-2 increases the risk of short-and long-term cardiovascular complications, many of which may be severe. Therefore, practicing clinicians and patients will embrace every tool that can be used to bring down this exposedness.
One of the things we learned some time ago is that, unfortunately, the first and second doses of COVID-19 vaccination may be associated with an increased risk of myocarditis (inflammation of the heart muscle) and pericarditis (inflammation of the pericardium,)(1, 2). This, of course, has given rise to considerable scientific and public interest and has been highlighted by anti-vaccination movements.
However, evidence shows that the risk of myocarditis is substantially higher after Covid-19 infection in unvaccinated individuals than the increase in risk observed following vaccination. Furthermore, vaccine-associated myocarditis is largely restricted to men younger than 40 years (3). Obviously, this still remains a matter of great concern.
Now, recently published data from the US shows that vaccination against COVID-19 is associated with fewer major adverse cardiovascular events (MACE) among people suffering from-Covid 19 when compared to unvaccinated patients. The researchers used the National COVID Cohort Collaborative (N3C) database, the largest national comprehensive database on COVID-19. The study results were published online in the Journal of the American College of Cardiology on February 20 (4). The results are presented in a letter and therefore I’m assuming this is not a peer reviewed paper.
The patients studied were between ages 18-90 and were initially infected with SARS-CoV-2 between March 1, 2020, and February 1, 2022. The follow-up time was 180 days from the start of the infection. The following vaccines were used: mRNA vaccines by Pfizer-BioNTech and Moderna, as well as vector vaccines by Johnson and Johnson.
The study addressed 1,934,294 patients, the mean age was 45.2 years, and 55.9% were women. A total of 195,136 patients were fully vaccinated, which interestingly is only 10.1 percent. The number of partially vaccinated was 22,707 (1.2%), and 1,716,451 (88.7%) were not vaccinated.
The median time to MACE after infection was 17 days, and the median time from the last vaccination to MACE was 212 days.
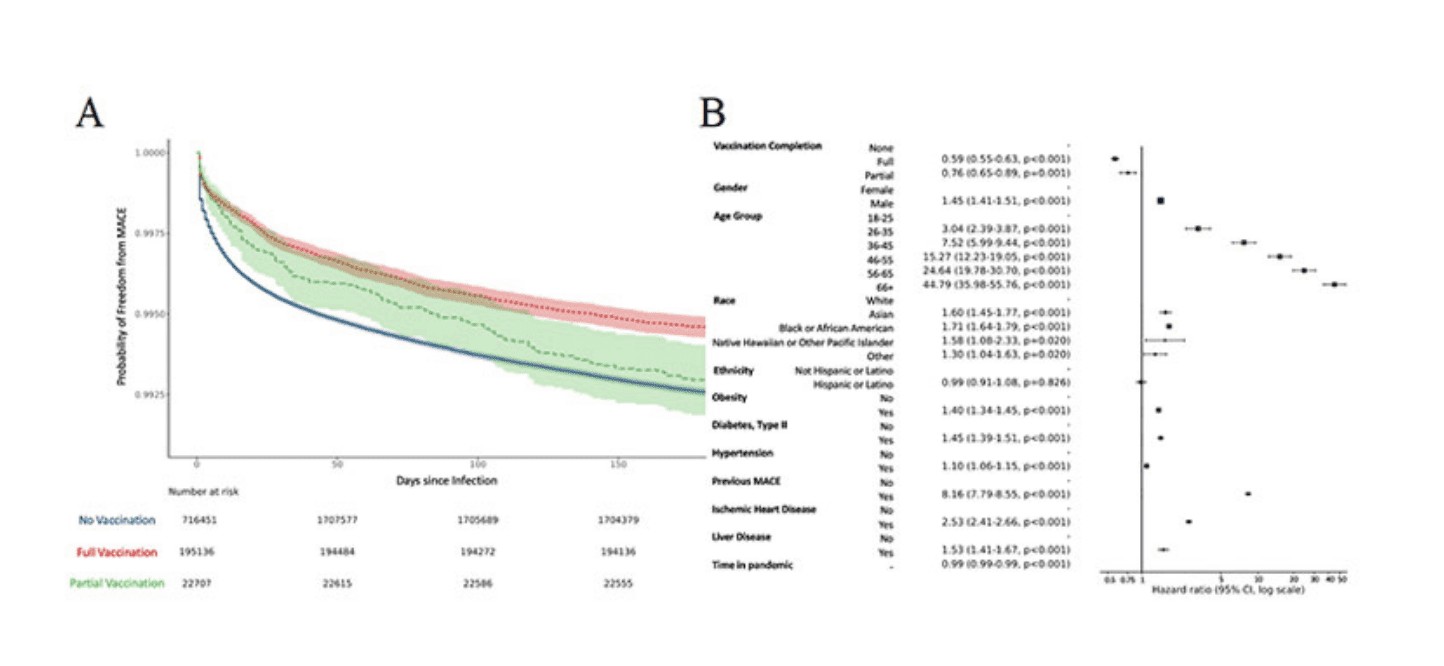
Overall, MACE was observed among 13,948 patients (0.72%): 12,733 cases occurred among non-vaccinated patients (0.74%), 160 in partially vaccinated patients (0.70%), and 1,055 in fully vaccinated patients (0.54%). In total, 3175 patients died after MACE.
Medscape Medical News reports that patients who were fully vaccinated had a 41% lower risk of experiencing a cardiac event compared to those who were not vaccinated. Partially vaccinated people had a 24% lower risk (5).
However, using the relative difference may be misleading. According to my own look at the numbers and assuming there is a protective effect of the vaccination, the number needed to treat will be 500. In other words, 500 patients need to be vaccinated to prevent one cardiac event from Cocid-19.
Taking into consideration that Covid-19 is a very common and widespread disease, the effect may indeed be huge. With an NNT of 500, vaccinating on million people may prevent 2.000 cardiac complications.
The results suggest that the difference between vaccinated and non-vaccinated people may be most pronounced in patients with a previous history of cardiovascular disease, patients with type 2 diabetes, lipid problems, liver disease, and obesity. Furthermore, the proposed benefits of vaccinations seem to increase with advancing age.
Of course, this is not a randomized trial, and we must remember that an association does not prove causality. However, the size of the study certainly suggests that Covid-19 vaccinations indeed do appear to provide protection against the cardiac complications of Covid-19. This may be particularly true for some subgroups of patients who are at higher risk.
According to one paragraph about the total number of events in the stated sample, there were fewer events for partially vaccinated people (160] than for fully vaccinated people (1055].
What does this tell us? It seems a bit contradictory, doesn’t it?
Hi Manny
You’ll have to take into account that the number of partially vaccinated people was much smaller than the number of fully vaccinated.
Hi Doc-happy to be corrected but wasn’t the risk of myocarditis raised most noticeably with the 2nd dose of mRNA vaccines especially in adolescent males? For this reason there was debate about the value of the 2nd vaccination in adolescents who were otherwise low risk for COVID-19 complications?
Thanks
Hi Neil
You’re right. According to the Italian/Lombardy study, the risk of myocarditis was highest following exposure to the second dose of the Moderna vaccine. Men beween 16-19 years old had the highest risk.
Interesting.
Hi Axel, interesting study, and thanks for the article.
I am wondering if the majority of the unvacc people in this study had an infection with the alpha variant since the date goes back to March 2020 and is therefore misleading, with regards to the later less severe variants. Maybe it’s corrected for in the study, or I’m misinterpreting, thank you for your great blog posts!
Best,
Thanks Kjartan.
A very good question indeed.
Considering the timeline you may be spot on.
This question is not addressed in the published letter.
The authors only state that they could not account for different SARS-CoV-2 variants underlying infection.
However, the unanswered question is to what extent the risk of cardiovascular complications differ between different SARS-CoV-2 variants.