Estimated reading time: 6 minutes
Carotid intima-media thickness (CIMT) is a relatively simple, noninvasive measure that uses ultrasound to detect the presence and extent of atherosclerosis in an artery.
Atherosclerosis, the underlying cause of coronary heart disease is characterized by an accumulation of lipids, white blood cells and cell debris in the inner layers of the arterial wall.

Atherosclerotic plaques may cause blockages in arteries supplying blood to vital organs such as the heart and brain. Plaque ruptures may cause blood clotting (thrombosis) leading to an abrupt closure of an artery. This may cause a heart attack (acute myocardial infarction) if it occurs in a coronary artery and stroke if it occurs in an artery to the brain.
Although some arteries are more susceptible to atherosclerosis than others, atherosclerosis is most often widespread, affecting most arteries in the body. Therefore, the amount of atherosclerosis in one artery will give a general idea about the quantity of atherosclerosis in other arteries as well.
The carotid arteries supply oxygenated blood to the brain. The pulse from the carotids may be felt on either side of the front of the neck just below the angle of the jaw.
Because atherosclerosis is a disease of the vessel wall, imaging the vessel wall is the ideal way to detect atherosclerosis. The carotid arteries are well suited for imaging because they are superficial and have limited movement.
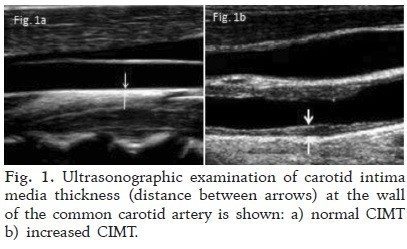
The wall of an artery consists of three layers, the intima, the media and the adventitia. Initially, atherosclerosis includes a gradual thickening of the intima and media layers. This thickening can be easily measured by direct visualization of the carotid arteries during ultrasound. As the two layers cannot be reliably distinguished, the combined intima-media thickness is measured. This measurement can provide valuable information about the amount of atherosclerosis present in the arterial wall.
Carotid Intima-Media Thickness (CIMT) Measurements
Atherosclerosis often starts at a young age, many years before the clinical symptoms of cardiovascular disease become manifest (1). Detecting and measuring atherosclerosis in asymptomatic individuals may be helpful to assess the risk of future cardiovascular events and to guide preventive measures.
CIMT measurement is one of the most widely used and best validated methods to detect early atherosclerosis. It correlates with many known risk factors for heart disease and the risk of future cardiovascular events.
Although ultrasound is the cheapest and most commonly used method to assess CIMT, other methods such as magnetic resonance imaging (MRI) can also be used.
B-mode, two-dimensional ultrasound with frequency ranges between 5 to 15 MHz is most often used to measure CMT. Various images are obtained to perform CIMT measurements, and the result is often a composite of different segments and angles.
Why Should Carotid Intima-Media Thickness (CIMT) Measurements Be Performed?
Although CIMT has been primarily used as a research tool in epidemiological and clinical trials, it is becoming more widely available and has the potential to play a significant role in clinical medicine. CIMT is relatively straightforward, safe and inexpensive. No radiation is involved, and no contrast is needed.
CIMT measurements are used to screen for atherosclerosis, assess the risk for future cardiovascular events, and analyze the effect of drug therapy.
Numerous prospective epidemiological studies have shown a correlation between CIMT and the risk of coronary artery disease (2,3). In the Kuopio Ischemic Heart Disease risk factor study, every 0.1 mm increment in CIMT was associated with an 11 percent increased likelihood of heart disease (3).
Cardiovascular risk is most often assessed by using risk calculators and risk scores (4). The method is based on providing the calculator with demographic and clinical information such as gender, race, family history, blood lipids, blood pressure, smoking and the presence or absence of diabetes. Based on population data, the risk calculator will provide a measure (percentage) of the risk of having heart disease or stroke in the next ten years.
Using risk calculators to quantify risk has several limitations. A high proportion of cardiovascular events occurs in people at low or intermediate risk (5). It has been proposed that CIMT may improve cardiovascular risk stratification by adding a direct measure of the amount of atherosclerosis present.
In one systematic review and meta-analysis, adding a one-time CIMT to the Framingham Risk Score was associated with a small improvement in 10-year risk prediction of first-time heart attack or stroke, but the authors concluded that this is unlikely to be of clinical importance (6).
It has been suggested that serial CIMT measurements may be more predictive of risk than one-time measures. However, one meta-analysis of available studies did not show CIMT progression as assessed be serial measurements to be associated with increased risk of cardiovascular events (7).
Whether using CIMT for risk stratification will transform into better outcome for patients is unknown. Therefore, routine use of CIMT is not recommended.
The 2010 American College of Cardiology Foundation/American Heart Association guidelines for the assessment of cardiovascular risk in asymptomatic adults gave CIMT a level IIa recommendation for cardiovascular risk evaluation in patients at intermediate risk, but no recommendations were made regarding low- or high-risk patients (8).
Carotid Intima-Media Thickness (CIMT) to Assess Drug Efficacy
CIMT has been frequently utilized in clinical trials to test the efficacy of cardiovascular drugs. However, it is important to acknowledge that a positive effect of a drug on CIMT is not necessarily translated into clinical benefit (e.g., lower risk of heart disease, stroke or death).
Numerous placebo-controlled trials have addressed the effects of lipid-lowering therapy on CIMT. Some of these studies clearly showed that progression of atherosclerosis was halted by statins (9,10,11,12). Furthermore, aggressive lipid-lowering therapy was shown to reduce CIMT progression more than moderate lipid lowering (13,14).
The effects of drugs used for the treatment of high blood pressure on CIMT have also been addressed in clinical trials. Metoprolol, amlodipine, and ramipril have all been shown to decrease CIMT progression (16,17,18).
What Is Normal Carotid Intima-Media Thickness (CIMT)?
CIMT above 1.0 mm is regarded as abnormal, and above 1.2 mm as considered high risk. However, the standard values need to be adjusted for age, gender and perhaps even ethnicity.
Typically, normal CIMT at age 10 is approximately 0.4 to 0.5 mm, while this progresses to 0.7 to 0.8 mm or more after the fifth decade of life (19).
The Clinical Usefulness of Carotid Intima-Media Thickness
CIMT has a few favorable characteristics as a screening tool for cardiovascular disease. It is noninvasive, safe and correlates with clinical outcome.
Another method commonly used to quantify atherosclerosis is coronary artery calcium score (19). The main disadvantage of this method compared to CIMT is the radiation exposure involved.
Appropriate reasons for using CIMT include patients at intermediate risk for coronary heart disease, and those with metabolic syndrome, diabetes, or a positive family history of premature heart disease (20).
Using CIMT to motivate lifestyle and behavioral change in people at risk may be warranted. Showing smokers with vascular disease images of their arteries to motivate smoking cessation may be beneficial, supporting the potential effectiveness of personalized biomarker feedback to improve lifestyle to reduce cardiovascular risk (21).
Thanks as always Dr Sigurdsson. 🙂
You’re welcome Hilary. Appreciate your interest and feedback as always.
Axel, great summary of the topic as usual.
I’ve been offering carotid IMT in my practice for the last 15 years.
It requires meticulous attention to measurement and recording and is not something that all cardiologists should offer because of that.
I am less enthusiastic about IMT/vasclar age over time and I rely much more heavily in my vascular screening on the presence of even small atherosclerotic plaque in the carotids to guide therapy.
However, we still need something that provide an “early warning” that patients will have premature plaque and this is all I have right now beyond the standard risk factors.
I summarized my experience on my blog a few years ago at //https://theskepticalcardiologist.com/2014/07/12/searching-for-subclinical-atherosclerosis-vascular-age/…
Some caveats I shared
*We don’t have good data sets on individuals under the age of 40 years. I offer CIMT to this group and extrapolate the good data but more studies are needed in this age range.
*We don’t have good data sets on ethnicities other than the African-americans and European and American whites.
*Multiple methods of CIMT recording and measurement have been published.
*I don’t find CIMT useful in individuals over the age of 70. Carotid plaque is much more helpful. Most men have carotid plaque by this age. If you don’t have any carotid plaque over the age of 70 years then you are in a very low risk category and are unlikely to benefit from statin or aspirin therapy.
…
What Hilary said…thanks Axel, as always. Your continued inputs are very much appreciated. As you might imagine from my earlier enquiry, I was keenly interested in the comment that CMIT “values need to be adjusted for age”. At 65 and with a CMIT score of 1.1, I was relieved (hopefully not falsely!?) by the footnote study’s conclusion that IMT for healthy participants >60 was 1.05…a sufficiently close result (in my VERY non-professional view!) to encourage and sustain my current abstention from statins; that, along with a long-standing focus on diet (very low sugar, low red meats, lotsa raw foods) and regular exercise (daily 1km swim) and a low (8) coronary calcium score. At some stage I will need to find a new cardiologist as I will not return to the fellow who seemed hell-bent on me taking statins!
Don.
As I see it, because of your healthy lifestyle choices you probably don’t have to worry too much although CIMT is in the upper range. Furthermore coronary calcium score is low for your age. I haven’t seen your lipid numbers though and don’t know about your family history but it certainly appears you are doing what you can to preserve your good health.
Hello again Alex
Just rec’d some update lipid numbers so I thought I’d pass them along…
Haemolysis … Nil
Icterus … Nil
Lipaemia … Nil
Fasting results…
Total Cholesterol … 5.3 mmol/L
Triglycerides … 0.6 mmol/L
HDL Cholesterol … 1.5 mmol/L
Non-HDL Cholesterol … 3.8 mmol/L
Cholesterol/HDL-C Ratio 3.5
Mmmm…must say my amateur understanding doesn’t leave me feeling all that great reading those numbers. Any comments…words of encouragement? Are we looking at a case for statins here…I sure hope not …
Argh! Axel…sorry about the name dyslexia!!
Hello Axel.
Would you treat an healthy individual with high risk for athersclerotic diseae and a positive findings on CIMT measurements with statins?
Guðný.
I would look at the bigger picture and go through all the risk factors such as smoking, family history, hypertension etc. and maybe use one of the risk calculators. CIMT could then provide additional information that might be helpful when deciding if to give statins or not in primary prevention, particularly if the individual is at intermediate risk.
27 yr old male just took a PAD screening, aorta and brachial normal but there is a thickening intima media for my age. What is my next step? How indicative is this of imminent problem, I have chest pain and leg pain and sometimes neck.